Uniform Healthcare Act Form
About this form
The Uniform Healthcare Act Form is an advance health care directive that allows individuals to outline their medical care preferences and appoint an agent to make health care decisions on their behalf. This form helps ensure that your wishes regarding medical treatment and end-of-life decisions are respected, reflecting your values and preferences in situations where you may no longer be able to communicate them yourself. It's important to note that this form should be adapted to comply with your state laws regarding healthcare directives and medical powers of attorney.
What’s included in this form
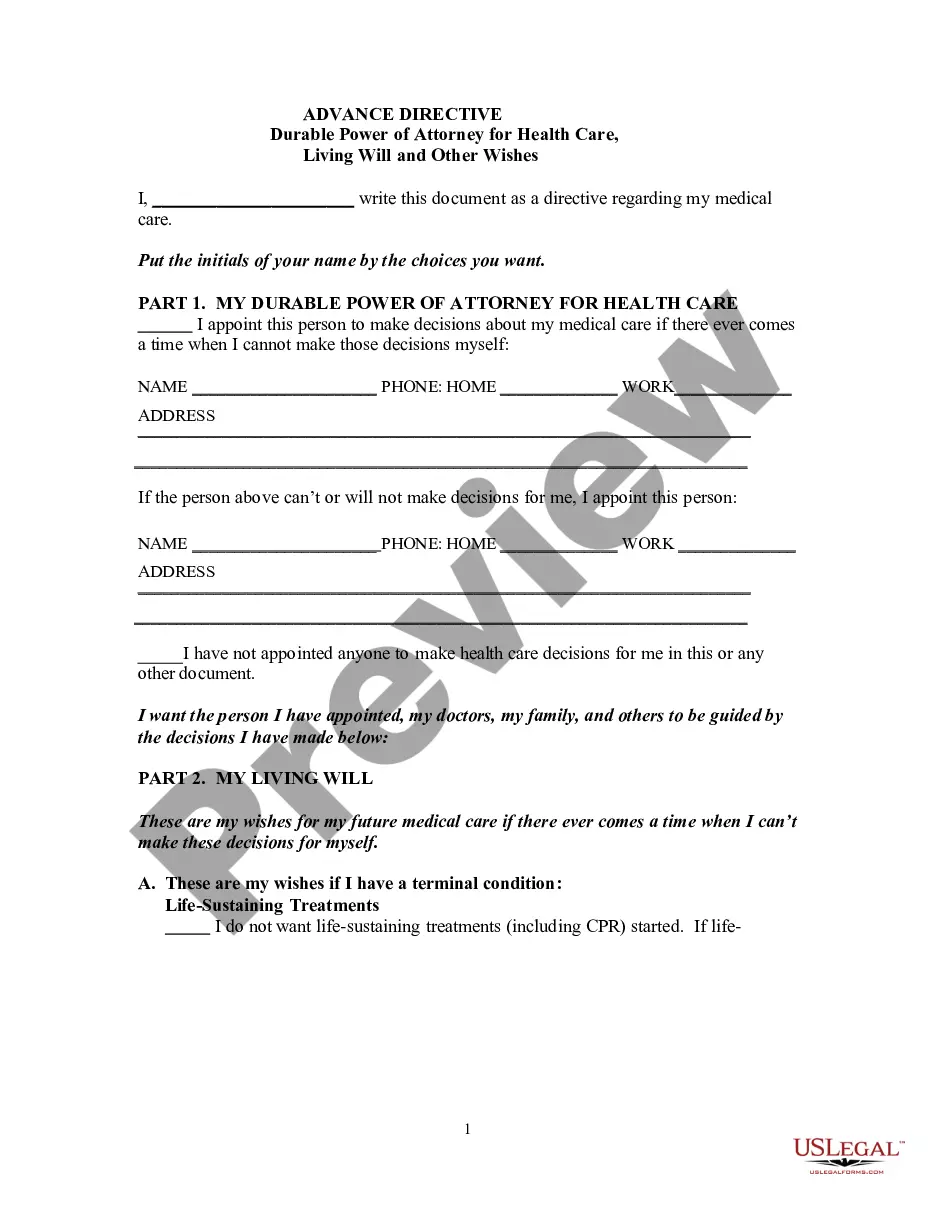
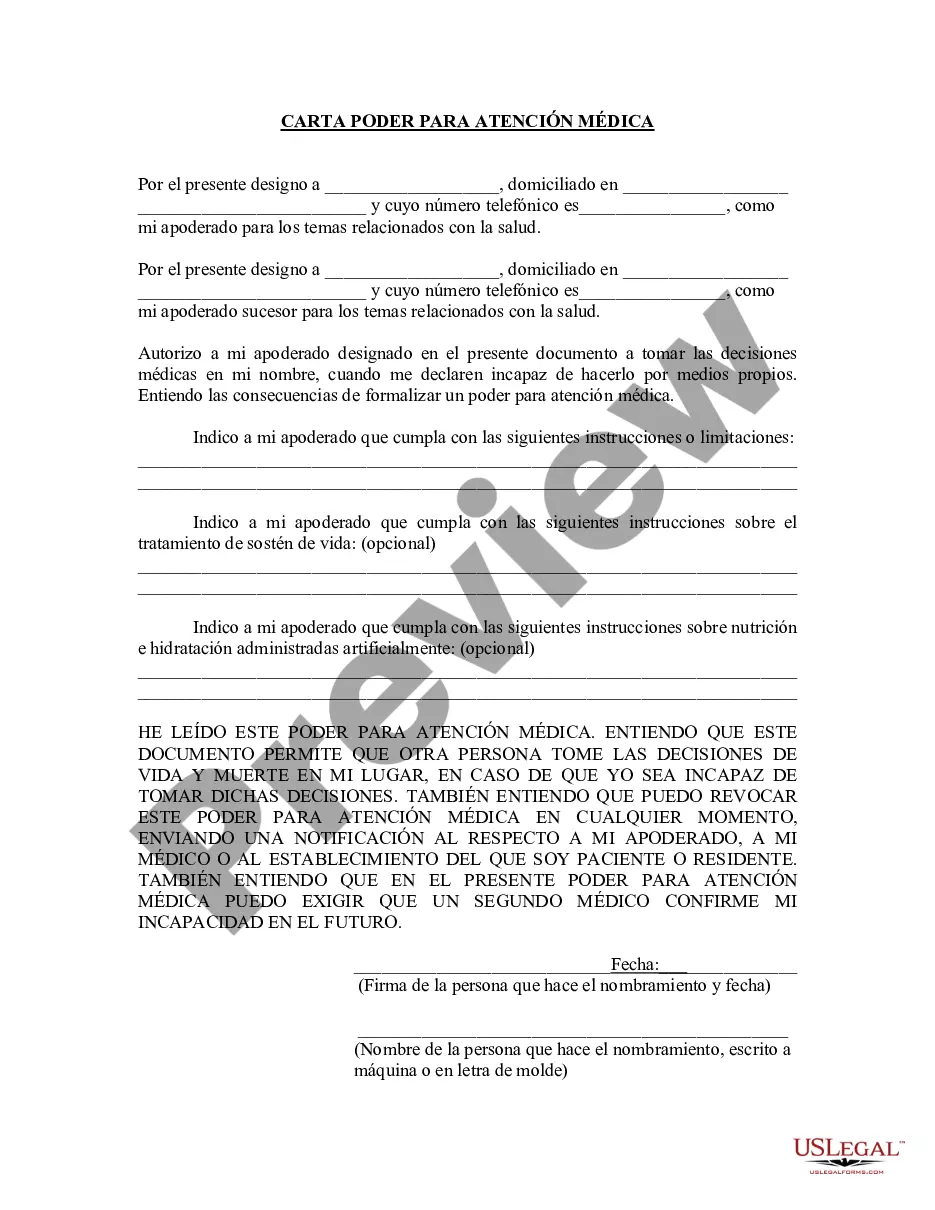
- Part 1: Power of attorney for health care to designate an agent who can make health care decisions on your behalf.
- Part 2: Specific instructions for health care, providing options for end-of-life decisions, artificial nutrition, and pain relief preferences.
- Part 3: Option to designate a primary physician responsible for your health care.
- Agent's authority to access medical information and make decisions according to your wishes.
- Witness or notarization requirements to validate the document.






When to use this form
This form should be used when you want to establish an advance directive for your health care, particularly in situations where you may be incapacitated and unable to make decisions for yourself. It is particularly important for individuals with chronic illnesses, those undergoing surgeries, or anyone seeking to specify their preferences for life-sustaining treatments.
Who can use this document
This form is suitable for:
- Adults who wish to outline their medical preferences in advance.
- Individuals wanting to appoint a trusted person as their health care agent.
- Those needing to clarify their wishes to family members and healthcare providers.
- People who may face medical decisions where their ability to communicate is compromised.
Steps to complete this form
- Designate your health care agent in Part 1, including their contact information.
- Specify any limitations on the agentâs authority or state preferences regarding health care decisions.
- In Part 2, indicate your wishes for end-of-life care, including options for artificial nutrition and pain relief.
- If desired, appoint a primary physician in Part 3.
- Sign and date the form, and ensure it is witnessed or notarized as required.
- Distribute copies of the completed form to your agent, physician, and any healthcare providers involved in your care.
Does this document require notarization?
Yes, this form must be notarized to be legally valid. Fortunately, US Legal Forms offers integrated online notarization, making it easy for you to have your document notarized securely via video call, ensuring compliance without the need for travel.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Common mistakes to avoid
- Not updating the form if your preferences or agent change.
- Failing to have the form witnessed or notarized, if required.
- Leaving sections blank that specify your wishes or preferences.
Advantages of online completion
- Convenience of completing the form from home without the need for a visit to an attorney.
- Editability allows you to customize the document to fit your specific needs and wishes.
- Access to reliable templates drafted by licensed attorneys, ensuring legal compliance.
- The advance healthcare directive is generally enforceable as long as it meets state legal requirements.
- It is crucial to ensure that the document complies with local laws to avoid any limitations on its use.
- Agents named in the directive have broad authority and must act in accordance with the wishes of the principal, considering their best interests.
Main things to remember
- The Uniform Healthcare Act Form allows you to specify your health care preferences and designate a decision-maker.
- It is important to ensure that the form complies with your state laws.
- Clear communication with your appointed agent is crucial to ensure your wishes are honored.
Looking for another form?

Form popularity
FAQ
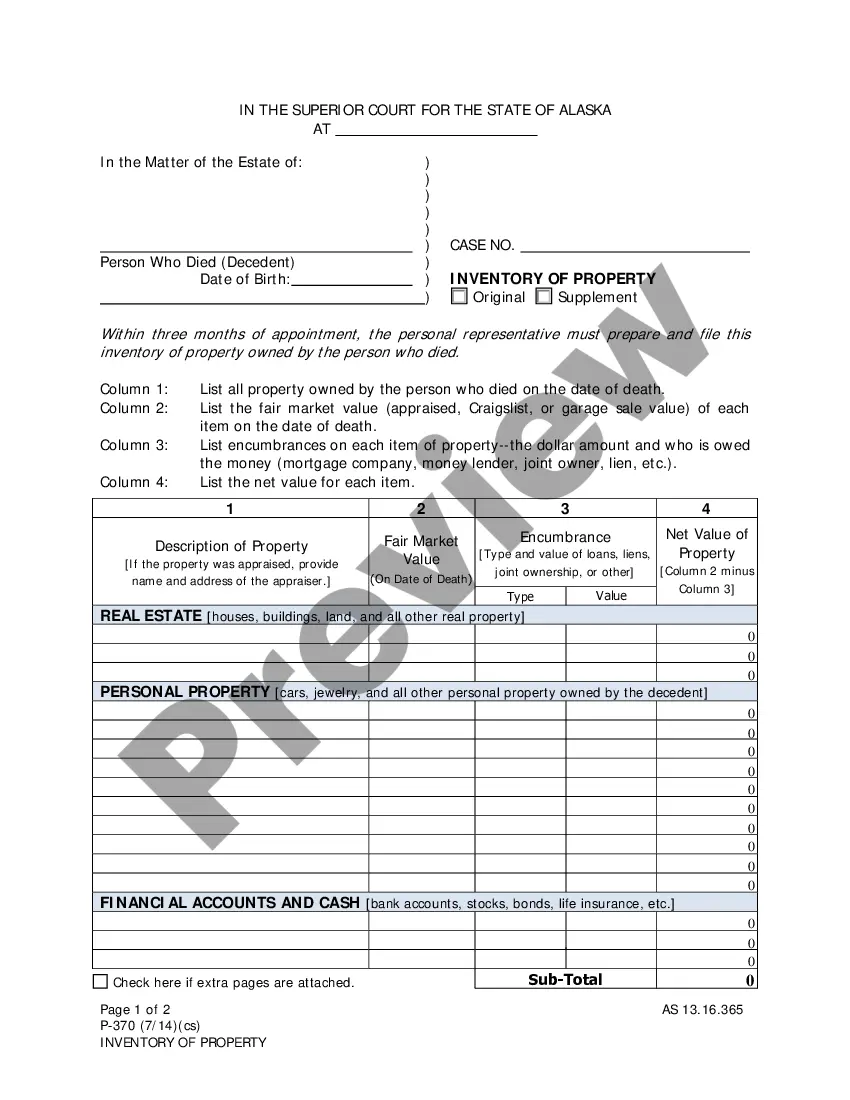
Health care decision means a decision made by a patient or the patient's agent, conservator, or surrogate, regarding the patient's health care, including the following: 27a2 Selection and discharge of health care providers and institutions, 27a2 Approval or disapproval of diagnostic tests, surgical procedures, and programs
Get the living will and medical power of attorney forms for your state, or use a universal form that has been approved by many states. Choose your health care agent. Fill out the forms, and have them witnessed as your state requires.
You can usually get advance directive forms from your state bar association, or from Caring Connection (part of the National Hospice and Palliative Care Organization). Additionally, when you are ready to fill out your advance directive, your health care team might be able to help.
Sign Your California Advance Directive in Front of Two Witnesses or a Notary Public. After you create your advance directive, you must sign your document and have it either signed by two witnesses or notarized. If you choose to have the document witnessed, neither of your witnesses may be: your health care agent.
Uniform Health-Care Decisions Act (UHCDA) is a uniform act drafted by the National Conference of Commissioners on Uniform State Laws in 1993.UHCDA also provides a form for executing a health-care power of attorney, for written instructions to a health-care provider, and even for making anatomical gifts.
Both the Uniform Health-Care Decisions Act (UHCDA) and the Uniform Guardianship and Protective Proceedings Act (UGPPA) advocate the inclusion of a decision-making standard that generally follows a three-step hierarchy in decision-making: (1) in accordance with the explicit instructions of the individual, (2) in
Review and complete the Advance Health Care Planning: Making Your Wishes Known Booklet. Complete An Advance Health Care Directive Form. Give a copy to your doctor, power of attorney and family. If necessary, complete a Provider Orders for Life Sustaining Treatment (POLST) Form.
The name and contact information of your healthcare agent/proxy. Answers to specific questions about your preferences for care if you become unable to speak for yourself. Names and signatures of individuals who witness your signing your advance directive, if required.
"Conservator" means a court-appointed conservator having authority to make a health care decision for a patient. 4615.