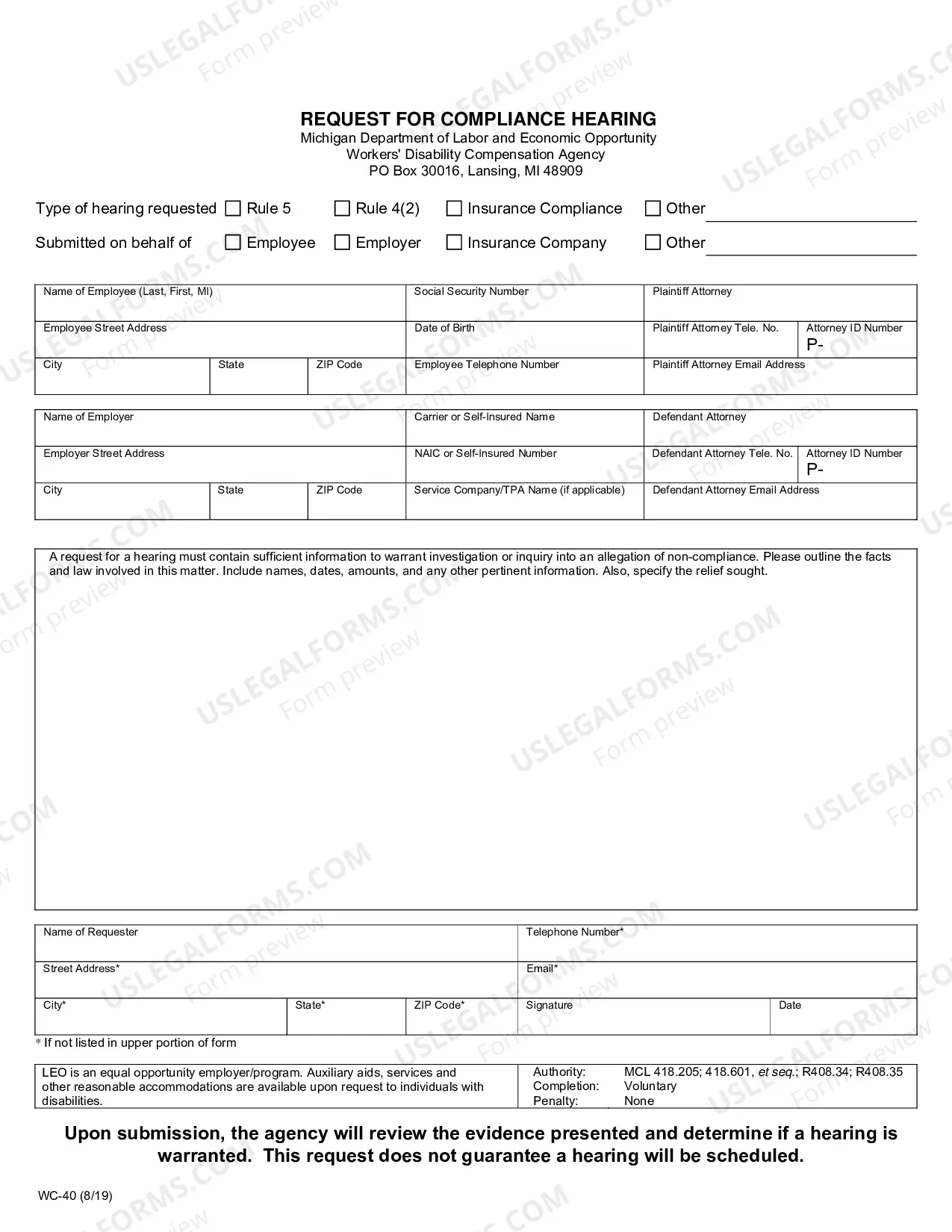
The Michigan Provider's Request for Reconsideration (fill-in form) is a document used by healthcare providers to appeal denied claims to the Michigan Department of Health and Human Services. This form is used to request a review of a claim to determine if it should be reconsidered for payment. The form provides an overview of the denied claim, the grounds for the appeal, and the requested remedy. The form is available in two versions: an individual provider version and a facility version. Both versions must be completed in full and submitted to the appropriate office. The form must be signed and dated by the provider submitting the request. Once submitted, the Michigan Department of Health and Human Services will review the request and make a determination on whether to approve or deny the reconsideration request.
Michigan Provider's Request for Reconsideration (fill-in form)
Instant download
This website is not affiliated with any governmental entity
Public form
Description
Provider's Request for Reconsideration (fill-in form)
How to fill out Michigan Provider's Request For Reconsideration (fill-in Form)?
If you’re looking for a method to suitably prepare the Michigan Provider's Request for Reconsideration (fill-in form) without employing a legal advisor, then you’re exactly in the right place.
US Legal Forms has established itself as the most comprehensive and esteemed repository of formal documents for every personal and business circumstance. Every piece of paperwork you find on our online platform is crafted in accordance with national and state laws, so you can be assured that your documents are in order.
Another significant benefit of US Legal Forms is that you never misplace the documents you acquired - you can access any of your downloaded templates in the My documents tab of your profile whenever you require it.
- Ensure the document you view on the page aligns with your legal circumstance and state laws by reviewing its text description or browsing through the Preview mode.
- Input the form title in the Search tab at the top of the page and select your state from the list to find an alternative template in case of any discrepancies.
- Repeat with the content verification and click Buy now when you are confident about the paperwork's compliance with all the requirements.
- Log in to your account and click Download. Create an account with the service and select the subscription plan if you do not have one yet.
- Utilize your credit card or the PayPal option to pay for your US Legal Forms subscription. The template will be accessible for download immediately after.
- Select the format in which you wish to receive your Michigan Provider's Request for Reconsideration (fill-in form) and download it by clicking the corresponding button.
- Upload your template to an online editor to complete and sign it swiftly or print it out to prepare your physical copy manually.

")