Illinois Release and Authorization
About this form
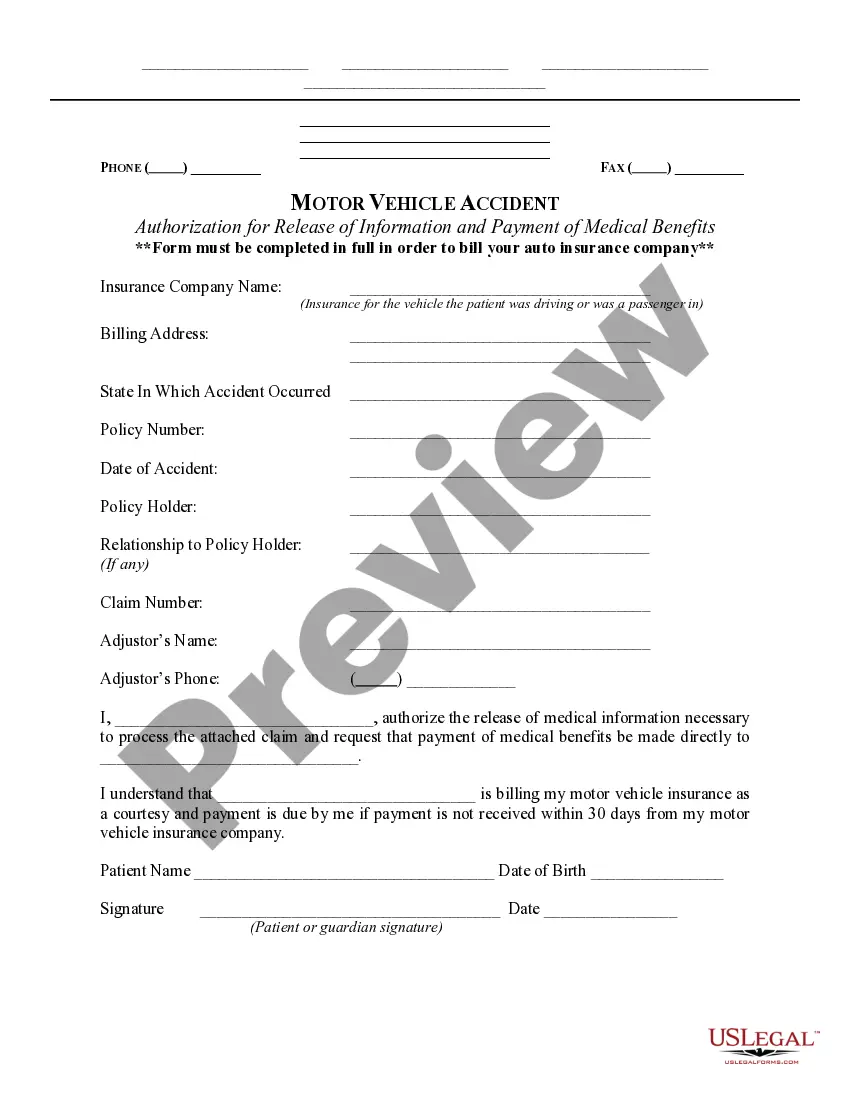
The Illinois Release and Authorization is a HIPAA authorization form specifically designed for the state of Illinois. This form allows individuals to authorize their healthcare providers to use or disclose their protected health information. Unlike similar forms, the Illinois version adheres to state-specific regulations while complying with federal laws outlined in the Health Insurance Portability and Accountability Act (HIPAA).
Key parts of this document
- Authorization: Names the healthcare provider and recipient of the information.
- Effective Period: Covers all past, present, and future periods of healthcare.
- Extent of Authorization: Allows release of the complete health record.
- Use: Describes permitted uses of the medical information.
- Termination: States the authorization remains in effect until the death of the patient.
- Revocation Rights: Explains the patient's right to revoke the authorization.



When this form is needed
This form is essential when a patient needs to allow their healthcare provider to share their health information with other individuals or organizations. Common situations include coordinating medical treatment, facilitating billing or claims payments, or authorizing information for legal or insurance purposes.
Who needs this form
- Patients who want to share their medical records with another healthcare provider.
- Individuals involved in legal matters requiring access to health information.
- Family members or personal representatives acting on behalf of the patient.
Completing this form step by step
- Identify the healthcare provider you are authorizing to share your information.
- Specify the individual or entity who will receive the protected health information.
- Provide your personal information, including name, address, telephone number, and date of birth.
- Sign and date the form to validate your authorization.
- Keep a copy for your records after submitting the form to your healthcare provider.
Does this form need to be notarized?
This form does not typically require notarization unless specified by local law. Ensure that you follow the instructions provided by your healthcare provider regarding any notarization requirements.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Avoid these common issues
- Failing to complete all required fields, which can delay processing.
- Not specifying the extent of authorization, leading to potential misunderstandings about what information can be disclosed.
- Overlooking the signature requirement, which invalidates the authorization.
Advantages of online completion
- Easy access: Download and complete the form anytime from anywhere.
- Editable: Fill in your information digitally, reducing the chance of errors.
- Secure: Your personal information is safely handled and stored.
Looking for another form?

Form popularity
FAQ
Authorization for release of information means the form prescribed by the agency for the purpose of authorizing the release of a confidential record, signed and dated by the person empowered to release the information.
A HIPAA authorization form, also known as a HIPAA release form, is a document that individual signs for their health provider before the entity may use or disclose their protected health information (PHI).
Usually, your health care provider must respond to your request for your record within 30 days of receiving your request. Generally, your health care provider must give you a copy in the format that you request if they are able to do so. You may have to pay a fee to get a copy of your record.
A Standard Document authorizing the release of protected health information to third parties, under the requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPAA).
Under the HIPAA Privacy Rule, healthcare providers, health plans, business associates, and others involved in administration of healthcare, may not share a patient's protected health information (PHI) without that patient's written authorization.
HIPAA Authorization is a document that authorizes the release of medical records which are protected under HIPAA. The authorization names designated representatives who may receive protected medical records, despite the privacy protections of HIPAA. HIPAA is an important piece of legislation.
By setting up a Release Authorization (ARI), you are giving customer service your permission to disclose information about your accounts to another person. Typically, this is used to give account access to a spouse or other family member.
A: ?Consent? is a general term under the Privacy Rule, but ?authorization? has much more specific requirements. The Privacy Rule permits, but does not require, a CE to obtain patient ?consent? for uses and disclosures of PHI for treatment, payment, and healthcare operations.