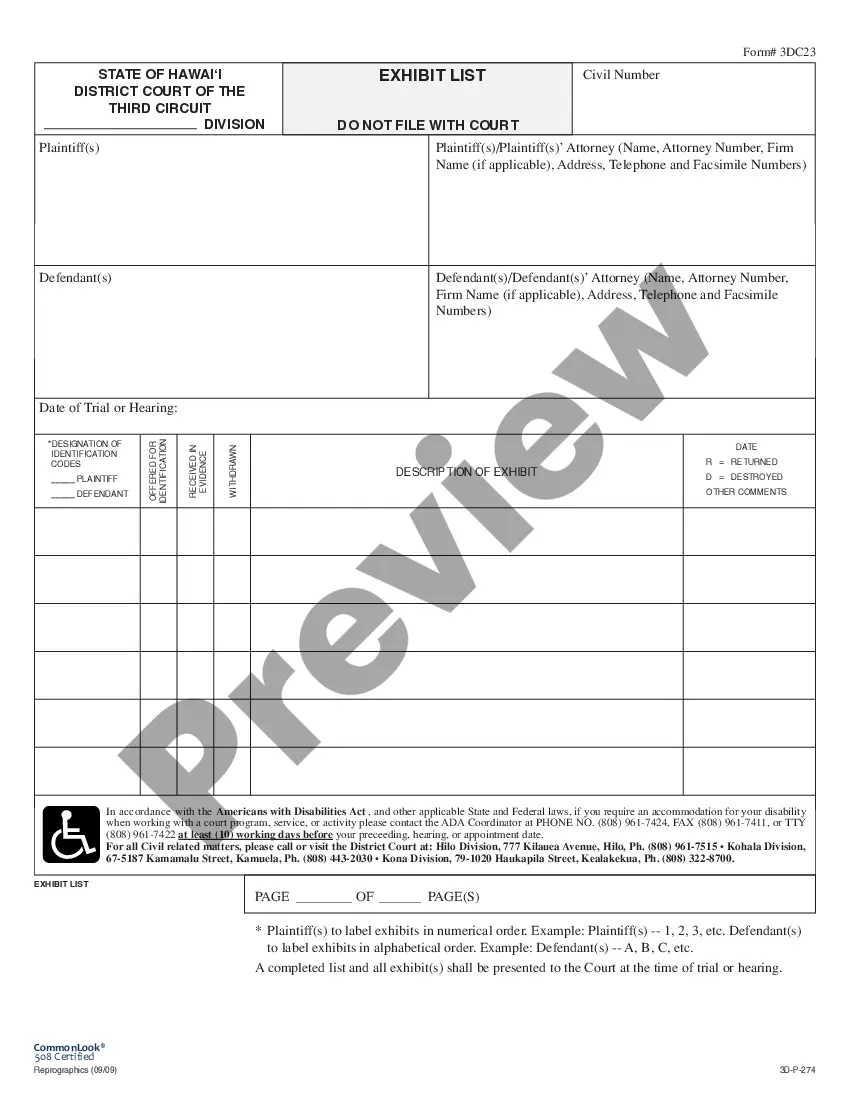
Election Form for Continuation of Benefits - COBRA
What this document covers
The Election Form for Continuation of Benefits - COBRA allows employees to elect to continue their health insurance coverage following certain events, such as job loss or qualifying life changes. This form differs from other health insurance forms as it specifically addresses COBRA regulations, ensuring that employees have the option to maintain their benefits for a limited time during transitions.
What’s included in this form
- Section for the effective date of coverage continuation.
- Options for different qualifying events, such as retirement and divorce.
- Details on dependent eligibility, including children reaching maximum age for coverage.
- Information regarding other insurance coverage that may affect benefits.
- Monthly premium rates based on selected plans and coverage levels.
- Instructions for payment and consequences of non-payment.







When this form is needed
This form should be used when an employee experiences a qualifying event, such as job termination, retirement, divorce, or the death of a spouse, and wishes to continue their health insurance benefits under COBRA. It is critical to submit this form within the required timeframe to ensure coverage continuity.
Who needs this form
This form is intended for:
- Employees who have lost their job or have been laid off.
- Individuals transitioning from active employment to retirement.
- Dependents of employees who are navigating divorce or bereavement.
- Eligible dependent children approaching age limits for coverage.
Steps to complete this form
- Fill in the effective date of coverage continuation.
- Indicate the qualifying event leading to coverage continuation.
- Provide information about other health insurance coverage, if applicable.
- Select the desired coverage option and complete the corresponding premium rates.
- Sign and date the form, ensuring all required fields are complete.
- Submit the form promptly, along with any initial premium payments, to avoid cancellation of coverage.
Is notarization required?
Notarization is not commonly needed for this form. However, certain documents or local rules may make it necessary. Our notarization service, powered by Notarize, allows you to finalize it securely online anytime, day or night.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Common mistakes to avoid
- Failing to submit the form within the required timeframe.
- Not providing accurate information about other health insurance coverages.
- Leaving required sections incomplete, which could delay coverage.
- Neglecting to sign and date the form before submission.
Why complete this form online
- Easy access to fill out and download at your convenience.
- Editable fields allow for accurate and timely information entry.
- Secure and reliable forms drafted by legal professionals ensure compliance.
Legal use & context
- This form is based on federal COBRA regulations ensuring employees can maintain health benefits.
- It is essential for compliance with employee rights regarding health coverage post-employment.
- Failure to adhere to proper usage can result in loss of benefits under COBRA.
Main things to remember
- The Election Form for Continuation of Benefits - COBRA is vital for maintaining health coverage after job loss or life changes.
- Understanding eligibility and timely submission are essential for coverage retention.
- Ensure careful completion of all fields to avoid processing delays.
Looking for another form?


Form popularity
FAQ
The Consolidated Omnibus Budget Reconciliation Act (COBRA) gives workers and their families who lose their health benefits the right to choose to continue group health benefits provided by their group health plan for limited periods of time under certain circumstances such as voluntary or involuntary job loss,
Leave a company with 20 or more employees, or have your hours reduced. Private sector and state or local government employers with 20 or more employees offer COBRA continuation coverage. Wait for a letter in the mail. Elect health coverage within 60 days. Make a payment within 45 days.
The insurance company. COBRA Election Notice. After receiving a notice of a qualifying event, the plan must provide the qualified beneficiaries with an election notice within 14 days. The election notice describes their rights to continuation coverage and how to make an election.
You may be eligible to apply for individual coverage through Covered California, the State's Health Benefit Exchange. You can reach Covered California at (800) 300-1506 or online at www.coveredca.com. You can apply for individual coverage directly through some health plans off the exchange.
You may be eligible to apply for individual coverage through Covered California, the State's Health Benefit Exchange. You can reach Covered California at (800) 300-1506 or online at www.coveredca.com. You can apply for individual coverage directly through some health plans off the exchange.
COBRA continuation coverage lets you stay on your employer's group health insurance plan after leaving your job. COBRA stands for the Consolidated Omnibus Budget Reconciliation Act. It's shorthand for the law change that required employers to extend temporary group health insurance to departing employees.
There are several other scenarios that may explain why you received a COBRA continuation notice even if you've been in your current position for a long time: You may be enrolled in a new plan annually and, therefore, receive a notice each year. Your employer may have just begun offering a health insurance plan.
With COBRA insurance, you're on the hook for the whole thing. That means you could be paying average monthly premiums of $569 to continue your individual coverage or $1,595 for family coveragemaybe more!
Assuming one pays all required premiums, COBRA coverage starts on the date of the qualifying event, and the length of the period of COBRA coverage will depend on the type of qualifying event which caused the qualified beneficiary to lose group health plan coverage.