Mississippi Response Form for ADA Request from Medical Practitioner
Description


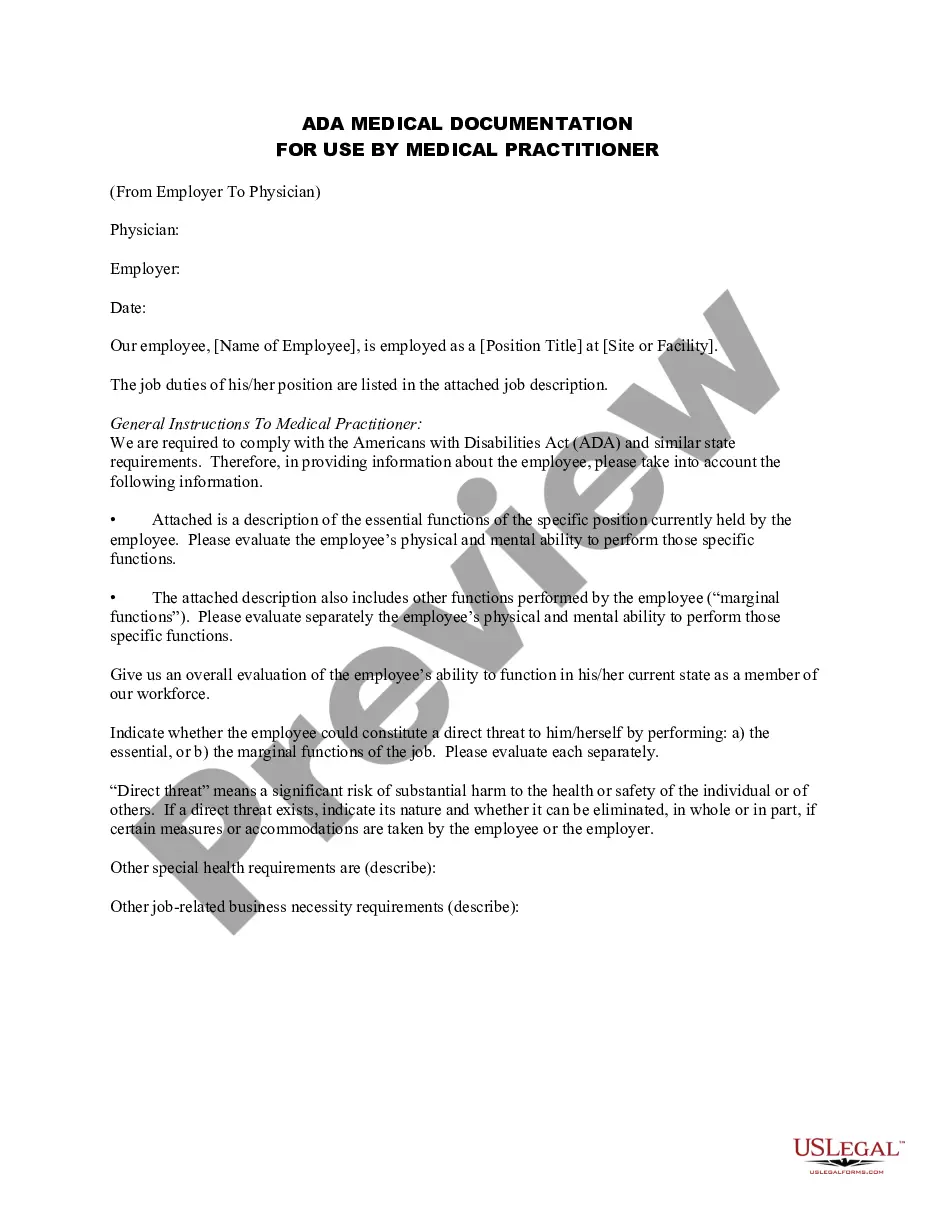
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Looking for another form?

How to fill out Response Form For ADA Request From Medical Practitioner?
Have you ever been in a location where you require documents for either business or personal purposes almost daily.
There are numerous legal document templates available online, but finding ones you can trust is challenging.
US Legal Forms offers thousands of template forms, including the Mississippi Response Form for ADA Request from Medical Practitioner, which is designed to meet state and federal requirements.
Utilize US Legal Forms, the most extensive collection of legal forms, to save time and prevent errors.
The service offers professionally crafted legal document templates that you can use for various purposes. Create an account on US Legal Forms and start simplifying your life.
- If you are already familiar with the US Legal Forms website and have an account, simply Log In.
- Then, you can download the Mississippi Response Form for ADA Request from Medical Practitioner template.
- If you do not have an account and wish to start using US Legal Forms, follow these steps.
- Select the form you need and ensure it is appropriate for your city/state.
- Use the Review button to examine the form.
- Read the description to verify that you have selected the correct form.
- If the form is not what you need, use the Search section to find the form that matches your needs and requirements.
- Once you find the right form, click Buy now.
- Choose the pricing plan you prefer, fill in the required information to create your account, and pay for the purchase using your PayPal or credit card.
- Select a convenient file format and download your copy.
- You can find all the document templates you have purchased in the My documents menu.
- You can obtain an additional copy of the Mississippi Response Form for ADA Request from Medical Practitioner at any time if needed.
- Just follow the necessary link to download or print the document template.
Form popularity
FAQ
The ADA requires employers to treat any medical information obtained from a disability-related inquiry or medical examination (including medical information from voluntary health or wellness programs (9)), as well as any medical information voluntarily disclosed by an employee, as a confidential medical record.
This questionnaire is part of an interactive process that is necessary in order to determine if your patient (our employee) has a disability recognized under the Americans With Disabilities Act, and, if so, what, if any, reasonable accommodation(s) are necessary and can be made that would enable your patient to perform
How to Handle an Employee's Request for an ADA AccommodationStep 1: Determine Whether the Employer Is Covered by the ADA.Step 2: Ensure a Policy and Procedure Exist for Handling Accommodation Requests.Step 3: Determine Whether the Employee with a Disability Is "Qualified"Step 4: Initiate the Interactive Process.More items...
There are various reasons why an employer may choose to deny an accommodation request made under the ADA. It is possible that by asking about your employer's reasons, you might be empowered to change the outcome of the situation.
There is no required procedure for employers to follow, or medical certification form that must be used to obtain medical information for ADA purposes. Also, there is no ADA-required time frame for employees to obtain medical information requested by an employer after a request for accommodation.
According to the EEOC, there is no specific amount of time that employers have to respond to an accommodation request, but they should respond as quickly as possible. Unnecessary delays in responding or implementing an accommodation can result in a violation of the ADA.
The ADA does not provide employers with unfettered discretion to decide what is reasonable. An employer may not rescind an existing reasonable accommodation, unless there is a material change in circumstances that warrants it.
Dear Mr./Ms. (Contact at Human Resources Department): I work at (Company Name) as a (Your Job Title) and have been in this position since (Date). I am writing to request that you provide (list accommodation needed here) as a reasonable accommodation under the ADA.
Dear Mr./Ms. (Contact at Human Resources Department): I work at (Company Name) as a (Your Job Title) and have been in this position since (Date). I am writing to request that you provide (list accommodation needed here) as a reasonable accommodation under the ADA.
Examples of reasonable accommodations include making existing facilities accessible; job restructuring; part-time or modified work schedules; acquiring or modifying equipment; changing tests, training materials, or policies; providing qualified readers or interpreters; and reassignment to a vacant position.