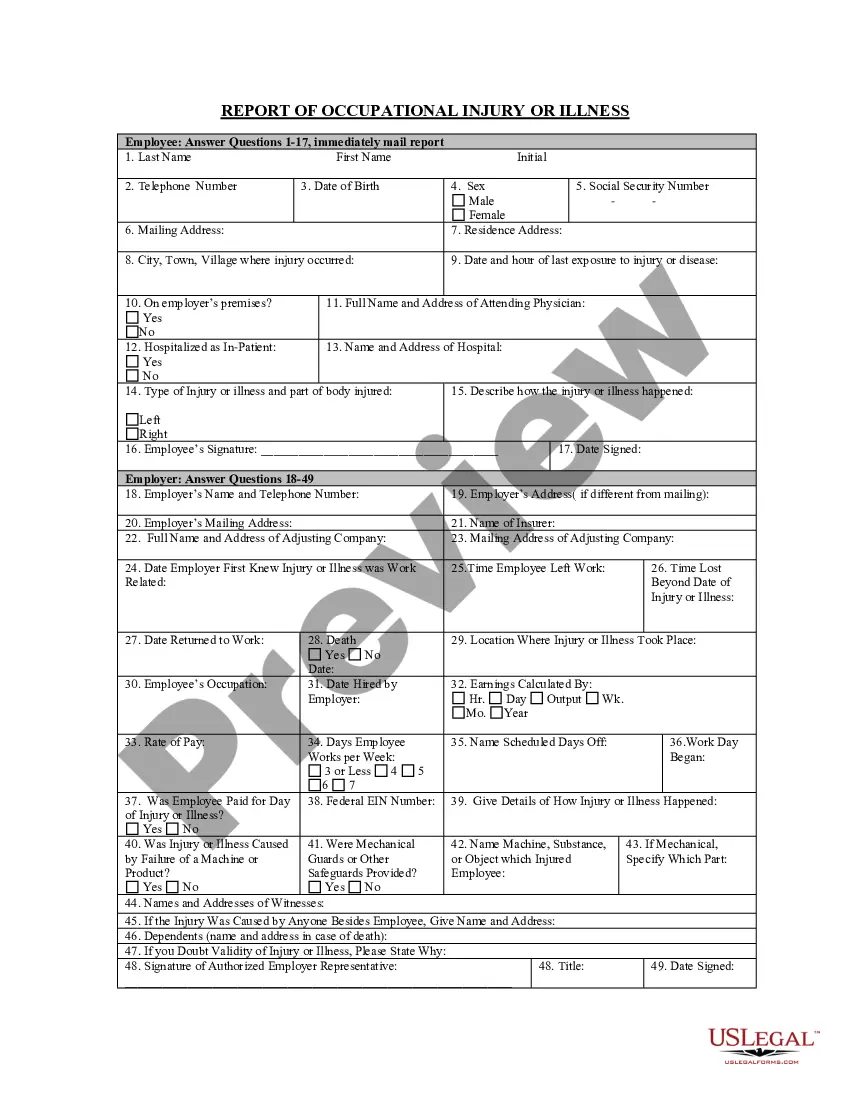
Report of Claimed Occupational Injury or Illness
Overview of this form
The Report of Claimed Occupational Injury or Illness is a crucial legal document that allows employees to formally report injuries or illnesses sustained in the workplace. This form serves to document the details of the incident, providing a clear and organized record for both the employee and employer. Unlike other forms, this report specifically focuses on occupational health issues and injuries, ensuring that claims are appropriately recognized and addressed.
Main sections of this form
- Name of Employee: The full name of the individual reporting the injury or illness.
- Address and Telephone: Contact information for the injured party.
- Date of Birth: The birth date of the employee, used for identification purposes.
- Date and Time of Event: When the injury or illness occurred.
- Description of Event: Detailed account of the circumstances leading to the reported injury/illness.
- Witness Information: Names of any witnesses who can corroborate the incident.
- Medical Treatment Information: Details about the medical treatment received, including dates and locations.
- Signature Fields: Signatures from the employee and supervisor verify the accuracy of the claims made.
When to use this form
This form is essential when an employee suffers an injury or illness at work that requires official documentation for claims or workplace compensation. It should be used in situations involving physical injuries, occupational diseases, or any incidents that could lead to a workers' compensation claim.
Who can use this document
This form is intended for:
- Employees who have experienced an occupational injury or illness.
- Employers needing to document workplace incidents for legal and insurance purposes.
- Human resources personnel managing employee health and safety records.
Instructions for completing this form
To complete the Report of Claimed Occupational Injury or Illness, follow these steps:
- Identify the employee's full name, address, and contact information.
- Provide the date and time when the injury or illness occurred.
- Clearly describe the events that led up to the injury or illness.
- Detail the nature of the injury or illness, specifying body parts affected.
- Include names of any witnesses to the event.
- Document any medical treatment received, including dates and providers.
- Ensure all required signatures from the employee and supervisor are completed.
Does this document require notarization?
This form does not typically require notarization unless specified by local law. Ensure that you check local regulations for any additional notarization requirements.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Avoid these common issues
- Failing to provide a detailed description of the event can lead to ambiguities.
- Not including witness information may weaken the claim.
- Omitting signatures can render the form invalid.
- Incorrectly filling out medical treatment details may delay processing.
Benefits of using this form online
- Convenience of completing the form online at any time.
- Editable templates that allow for clear, organized documentation.
- Access to attorney-drafted forms ensures compliance with legal standards.
- Use of this form can support claims for workersâ compensation benefits.
- Accurate completion is essential for legal enforceability in insurance claims.
What to keep in mind
- The Report of Claimed Occupational Injury or Illness is vital for documenting workplace injuries and illnesses.
- Providing complete and accurate information on this form is essential for a valid claim.
- Both the employee and employer must sign the report for it to be official.
Looking for another form?
Form popularity
FAQ
There is no specific time limits for OWCP to process your CA-7 other that it should be done as quickly as possible but it has been my experience that if there are no other issues going on with your claim and they do not dispute the CA-7 it usually takes 2-4 weeks for them to process and issue check or direct deposit.
Continuation of Pay (COP) is a special leave category which entitles employees to have their regular pay continued with no charge to their own leave for up to 45 calendar days (this includes weekends, holidays, and non workdays) of disability and/or medical treatment that follows an on the job injury.
Immediately Make A Work Injury Accident Report If you suffer a work-related injury or illness, immediately report it to your supervisor. If the injury or illness has gradually worsened over time (such as carpal tunnel syndrome), report it as soon as you think it was caused by your job.
If there is a serious injury or illness, a death or a dangerous incident, you must report it to us immediately on 13 10 50 as an urgent investigation might be needed. Incidents can be notified 24 hours a day, 7 days a week by calling 13 10 50.
How do I file a claim? You need to complete either form CA-1, "Federal Employee's Notice of Traumatic Injury and Claim for Continuation of Pay/Compensation" or form CA-2 "Notice of Occupational Disease and Claim for Compensation".
Report the accident to your employer, even if you think you are not seriously hurt. By reporting the accident, you protect yourself against the employer who might claim that you were injured away from the workplace. If possible, report the accident in writing or in the presence of a reliable witness.
What does an insurance carrier not do after it receives the first report of injury? Contact employees for medical records.
Avoid fines by reporting injuries right away An additional benefit of reporting injuries right away is avoiding fines. Even if a claim isn't compensable, insurers and ultimately employers in some cases face fines for late denial of liability if claims aren't reported on time.
The Employer's First Report of Injury or Illness provides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested.