Authorization to Use or Disclose Protected Health Information
What this document covers
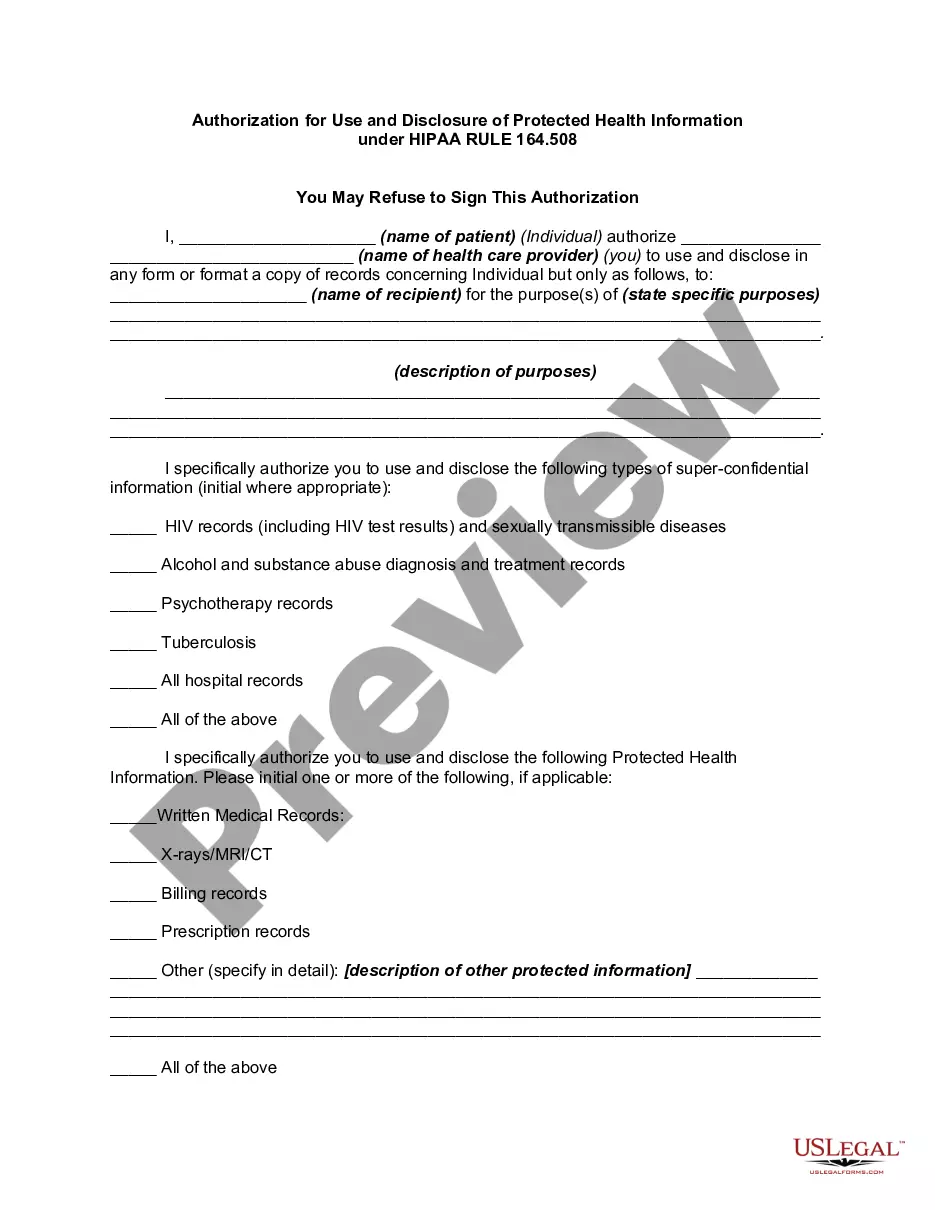
The Authorization to Use or Disclose Protected Health Information form allows individuals to provide consent for the use and sharing of their protected health information. This form is essential for managing healthcare privacy and ensures that individuals control who accesses their health records, including sensitive information such as psychiatric and HIV/AIDS records. Unlike other consent forms, this document specifically targets the disclosure of medical and health-related information, aligning with federal and state privacy laws.
Key components of this form
- Identification of the individual providing consent.
- Specific types of health information to be disclosed, such as lab results and x-rays.
- Individuals or entities authorized to receive the disclosed information.
- Duration of the authorization.
- Statement regarding the individual's rights related to the consent.






When this form is needed
This form should be used when an individual needs to grant permission for a healthcare provider or organization to share their protected health information with another party. Common situations include transferring medical records to a new healthcare provider, allowing family members to access health information, or participating in research studies that require data collection from health records.
Intended users of this form
- Patients who want to disclose their health information to other healthcare providers.
- Individuals participating in clinical trials who must allow researchers to access their health data.
- Caregivers seeking access to a loved one's health records.
- Anyone needing to authorize the release of sensitive health information for legal or administrative purposes.
Completing this form step by step
- Begin by stating your full name and contact information.
- Specify the types of protected health information you are allowing to be disclosed.
- Clearly indicate the names of the individuals or organizations authorized to access your information.
- Set a start and end date for the authorization period.
- Sign and date the form to validate your consent.
Notarization requirements for this form
This form usually doesn’t need to be notarized. However, local laws or specific transactions may require it. Our online notarization service, powered by Notarize, lets you complete it remotely through a secure video session, available 24/7.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Typical mistakes to avoid
- Failing to specify all types of health information that may be disclosed.
- Not including clear dates for the authorization period.
- Allowing disclosure to individuals or organizations not directly involved in your care.
Why complete this form online
- Convenient downloading and printing from any location.
- Easy modification to meet specific needs or circumstances.
- Access to attorney-drafted templates ensures compliance with current laws.
Legal use & context
Using this authorization form helps protect your rights under HIPAA while specifying how your health information can be used. It is important to understand that this form is only valid if proper procedures are followed regarding consent and disclosure.
Key takeaways
- The Authorization to Use or Disclose Protected Health Information is essential for managing personal health data sharing.
- Proper completion of this form ensures compliance with legal standards for health information disclosure.
- Understanding who should use this form helps protect patient privacy and confidentiality.
Looking for another form?
Form popularity
FAQ
It is important to emphasize the difference between a use and a disclosure of PHI. In general, the use of PHI means communicating that information within the covered entity.Disclosure - The release, transfer, access to, or divulging of information in any other manner outside the entity holding the information.
There are a few scenarios where you can disclose PHI without patient consent: coroner's investigations, court litigation, reporting communicable diseases to a public health department, and reporting gunshot and knife wounds.
However, PHI can be used and disclosed without a signed or verbal authorization from the patient when it is a necessary part of treatment, payment, or healthcare operations. The Minimum Necessary Standard Rule states that only the information needed to get the job done should be provided.
No, you should not sign the HIPAA authorization for the release of your medical records. Often, the insurance company will act as though they cannot begin to decide how much money to offer you until they have all of your medical records.
The law requires that a HIPAA authorization form contain specific core elements to be valid. These elements include: A description of the specific information to be used or disclosed. The name or other specific identification of the person(s), or class of persons, authorized to make the requested use or disclosure.
Generally speaking, covered entities may disclose PHI to anyone a patient wants. They may also use or disclose PHI to notify a family member, personal representative, or someone responsible for the patient's care of the patient's location, general condition, or death.
In general, a covered entity may only use or disclose PHI if either: (1) the HIPAA Privacy Rule specifically permits or requires it; or (2) the individual who is the subject of the information gives authorization in writing. We note that this blog only discusses HIPAA; other federal or state privacy laws may apply.
An authorization is a detailed document that gives covered entities permission to use protected health information for specified purposes, which are generally other than treatment, payment, or health care operations, or to disclose protected health information to a third party specified by the individual.
A covered entity may disclose protected health information to the individual who is the subject of the information. (2) Treatment, Payment, Health Care Operations. A covered entity may use and disclose protected health information for its own treatment, payment, and health care operations activities.