Employee Application for FMLA
What this document covers
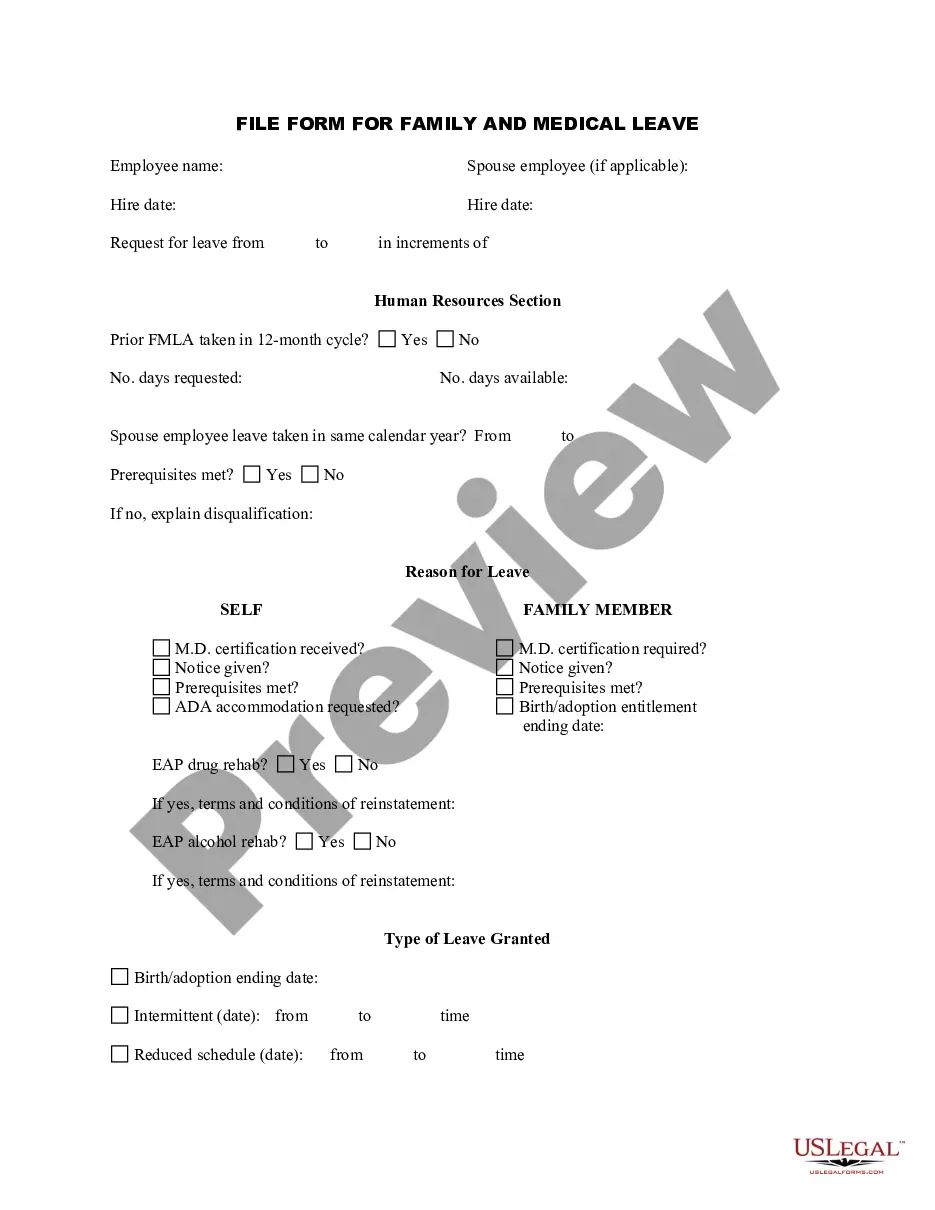
The Employee Application for FMLA is a formal request made by employees seeking Family and Medical Leave under the Family and Medical Leave Act (FMLA). This form allows employees to outline the reasons for requesting a leave of absence, whether for their own health conditions or to care for a family member. Unlike general leave request forms, this application specifically addresses the provisions of the FMLA, ensuring that the employee's rights are protected while enabling the employer to manage their workforce effectively during the employee's absence.
Key parts of this document
- Employee Information: Includes the employee's name, date of hire, and contact details.
- Reason for Leave: Checkboxes to indicate the reason for the leave, whether for birth, adoption, or a serious health condition.
- Medical Information: Sections to specify the nature of the medical condition and confirm hospitalization requirements.
- Intermittent Leave Request: Options to apply for leave that is not continuous, including potential arrangements with the employer.
- Employee Signature: A declaration for the employee's understanding of the leave policies under FMLA.


When this form is needed
This form should be used when an employee needs to take time off from work for valid medical reasons covered under the FMLA. Common scenarios include:
- Giving birth or adopting a child.
- Recovering from a serious health issue requiring extended medical care.
- Providing care for a seriously ill family member.
Intended users of this form
This form is intended for:
- Employees eligible for FMLA leave, typically those working for covered employers for at least 12 months.
- Workers dealing with their own serious health conditions or those of their family members.
- Individuals seeking legal protection for job security during extended medical absences.
How to prepare this document
- Fill in personal details such as your name and date of hire at the top of the form.
- Check the box corresponding to the reason for your leave from the provided options.
- If applicable, provide detailed information about your medical condition, including whether hospitalization is necessary.
- Specify if you are requesting continuous or intermittent leave and discuss any alternatives with your manager.
- Sign and date the form to authenticate your request before submitting it to your employer.
Is notarization required?
In most cases, this form does not require notarization. However, some jurisdictions or signing circumstances might. US Legal Forms offers online notarization powered by Notarize, accessible 24/7 for a quick, remote process.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Avoid these common issues
- Failing to provide complete or accurate medical information.
- Not understanding the FMLA policies before completing the form.
- Omitting the reason for leave or checking multiple unclear options.
- Not signing the form, missing this critical step for validity.
Benefits of using this form online
- Easy to fill out and edit, allowing for quick updates and corrections.
- Access to expert-validated content ensures compliance with legal standards.
- Save and download options available for easy record-keeping and future reference.
- Streamlined submission processes with guided instructions enhance user experience.
Legal use & context
- This form is crucial for rights under the Family and Medical Leave Act (FMLA).
- Using this form properly secures job protection while on authorized leave.
- Misinformation or submission of incomplete forms may lead to legal issues or denial of leave.
Looking for another form?
Form popularity
FAQ
How Do I Request FMLA Leave? To take FMLA leave, you must provide your employer with appropriate notice. If you know in advance that you will need FMLA leave (for example, if you are planning to have surgery or you are pregnant), you must give your employer at least 30 days advance notice.
Dear (Supervisor / HR Manager): Please be advised that I hereby request an FMLA leave for a period of (number of weeks) in connection with my serious health condition. The leave is to start on (date). Attached is my medical note reflecting the need for FMLA leave.
Step 1: Determine eligibility. There are two questions that need to be answered here. Step 2: Establish the qualifying reason. Step 3: Provide eligibility notice. Step 4: Provide request for medical certification. Step 5: Provide designation notice. Step 6: Leave is taken. Step 7: Return to work and reinstatement.
Dear name, I am writing this letter to inform you that I need to take sick leave from work. I will need to remain off work until date. I've included a letter from my doctor to confirm that I need to take that amount of time off to fully recover.
Understand your legal rights regarding time off and pay. Make the request in person. Give sufficient advance notice. If possible, work with your boss to develop an agreeable plan. Keep track of relevant paperwork.
The FMLA permits employers to request a doctor's note or medical certification when an employee first requests leave under the FMLA. If the employee is on extended leave, a doctor's note can be requested every 30 days.
Work for a covered employer; have worked 1,250 hours during the 12 months prior to the start of leave; ( special hours of service rules apply to airline flight crew members )
In order to be eligible to take leave under the FMLA, an employee must (1) work for a covered employer, (2) work 1,250 hours during the 12 months prior to the start of leave, (3) work at a location where 50 or more employees work at that location or within 75 miles of it, and (4) have worked for the employer for 12
If you are providing care for a family member and completing form WH-380-F, you will be required to take the FMLA form to your family member's health-care provider. Your healthcare provider is required by law to provide only factual information on this form.