Rhode Island Revocation of Authorization To Use or Disclose Protected Health Information
Description


How to fill out Revocation Of Authorization To Use Or Disclose Protected Health Information?
US Legal Forms - one of the largest repositories of legal documents in the USA - offers a plethora of legal form templates that you can download or print.
By utilizing the site, you can access thousands of forms for both business and personal purposes, organized by categories, states, or keywords.
You can locate the most recent versions of forms such as the Rhode Island Revocation of Authorization To Use or Disclose Protected Health Information within moments.
Review the form description to confirm that you have chosen the correct document.
If the form does not meet your requirements, utilize the Search box at the top of the screen to find one that does.
- If you already possess a subscription, Log In and retrieve the Rhode Island Revocation of Authorization To Use or Disclose Protected Health Information from your US Legal Forms library.
- The Acquire button will be visible on every form you view.
- You will have access to all previously saved forms in the My documents section of your account.
- If this is your first time using US Legal Forms, here are simple instructions to help you begin.
- Ensure you have selected the appropriate form for your city/region.
- Select the button to examine the form's content.
Form popularity
FAQ
Marketing Activities: A covered entity must obtain an individual's authorization prior to using or disclosing PHI for marketing activities. Marketing is considered any message or statement to the public in an effort to get them to use or seek more information about a product or service.
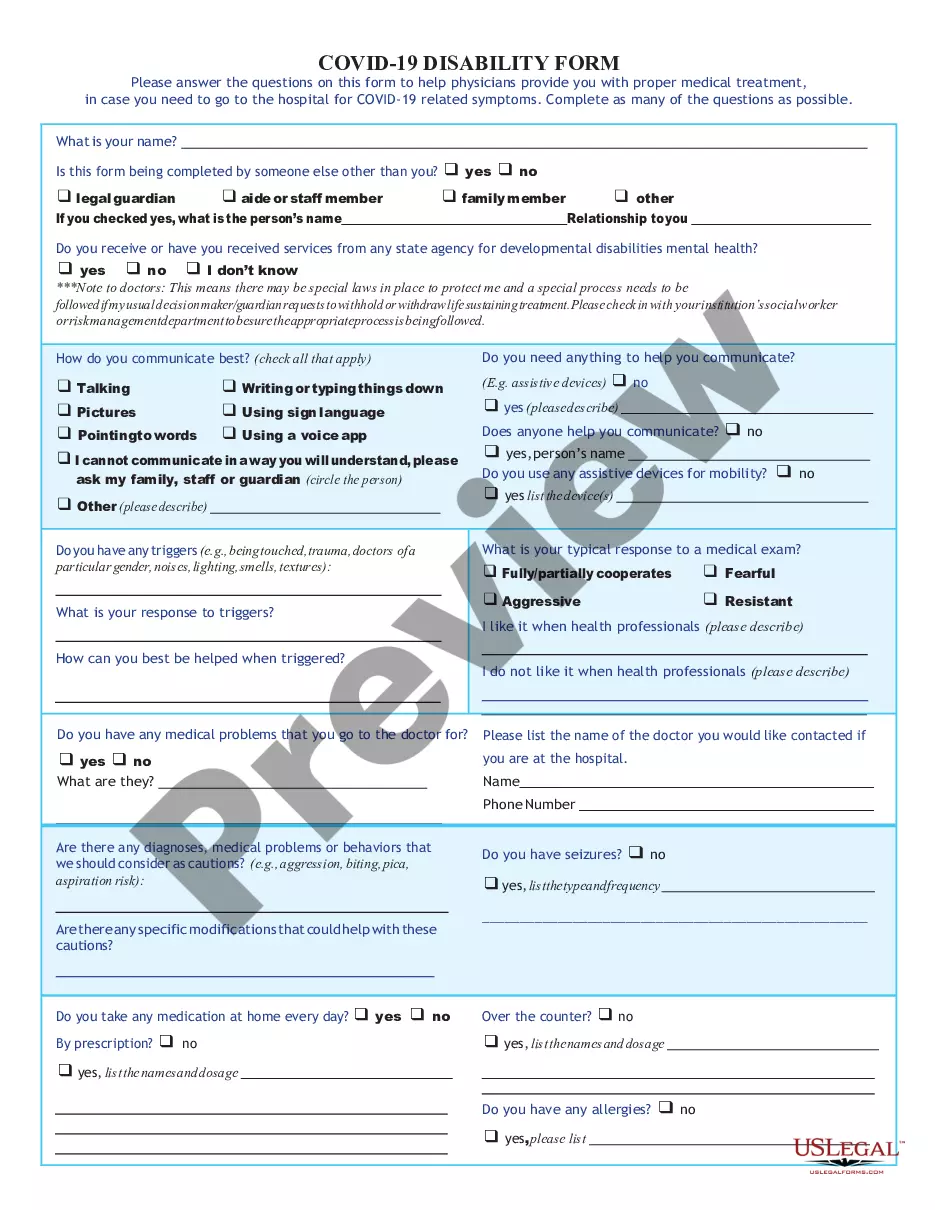
A HIPAA authorization is a detailed document in which specific uses and disclosures of protected health are explained in full. By signing the authorization, an individual is giving consent to have their health information used or disclosed for the reasons stated on the authorization.
Covered entities may disclose protected health information that they believe is necessary to prevent or lessen a serious and imminent threat to a person or the public, when such disclosure is made to someone they believe can prevent or lessen the threat (including the target of the threat).
Covered entities may disclose protected health information that they believe is necessary to prevent or lessen a serious and imminent threat to a person or the public, when such disclosure is made to someone they believe can prevent or lessen the threat (including the target of the threat).
With limited exceptions, the HIPAA Privacy Rule gives individuals the right to access, upon request, the medical and health information (protected health information or PHI) about them in one or more designated record sets maintained by or for the individuals' health care providers and health plans (HIPAA covered
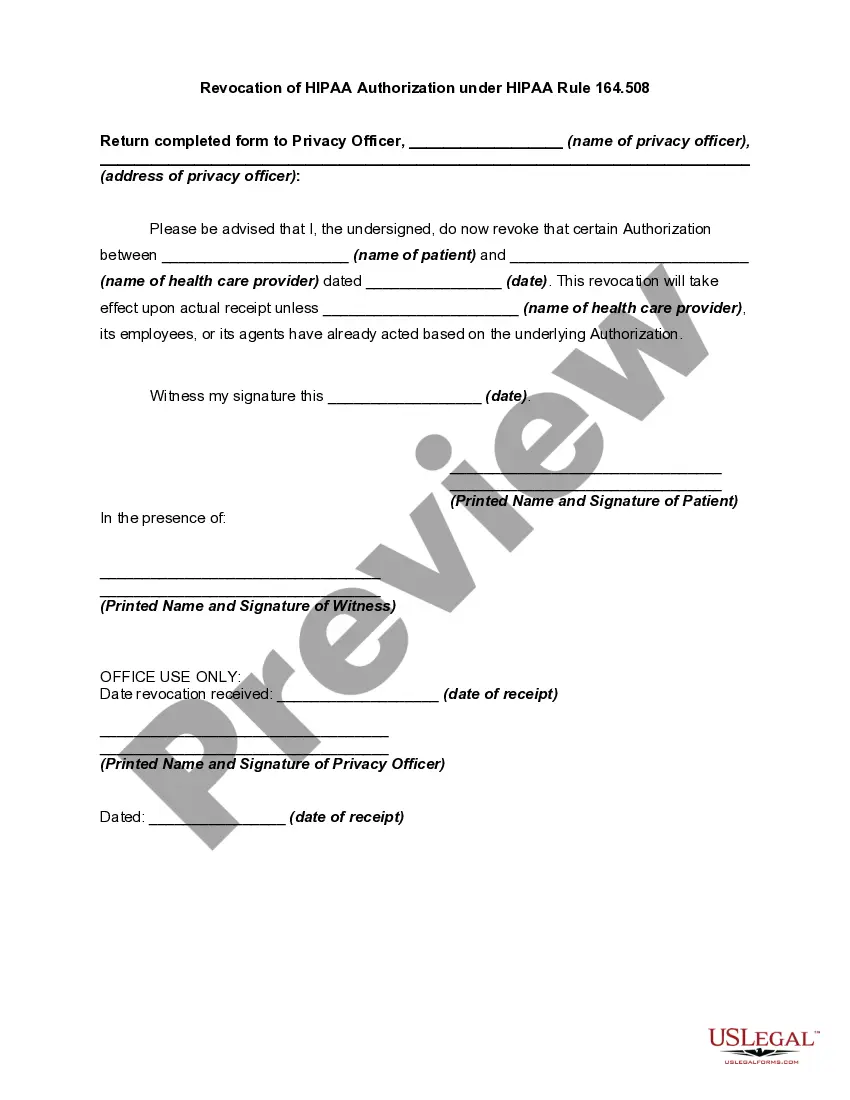
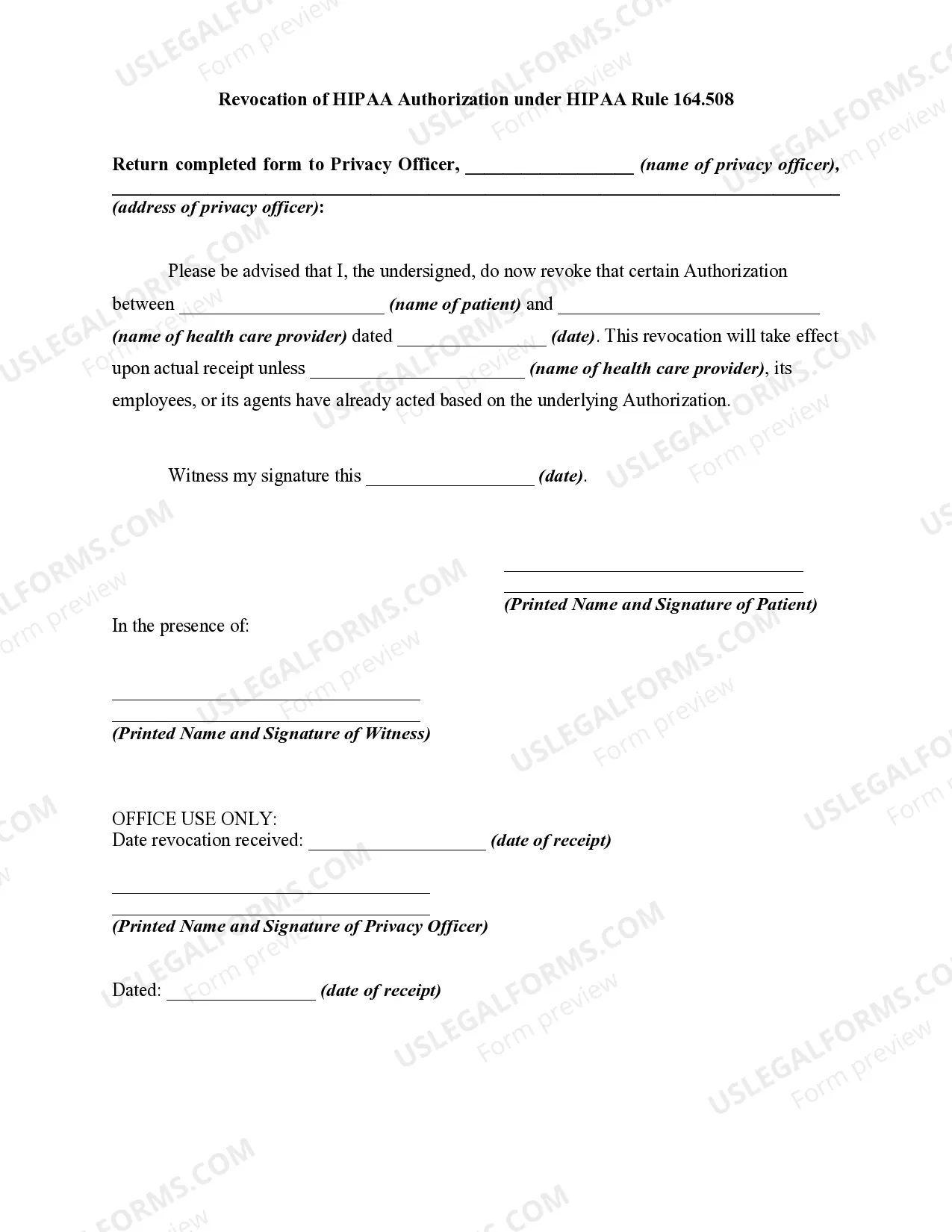
An authorization is a detailed document that gives covered entities permission to use protected health information for specified purposes, which are generally other than treatment, payment, or health care operations, or to disclose protected health information to a third party specified by the individual.
Health information such as diagnoses, treatment information, medical test results, and prescription information are considered protected health information under HIPAA, as are national identification numbers and demographic information such as birth dates, gender, ethnicity, and contact and emergency contact
Generally, an authorization provides the authority for a doctor's release of PHI for specified purposes, which are generally other than treatment, payment, or healthcare operations, or, to disclose protected health information to a third party specified by the individual.
We may disclose your PHI as authorized to comply with workers' compensation laws and other similar programs. Threats to Health or Safety. We may disclose limited PHI if we believe it is necessary to prevent or lessen a serious and imminent threat to you or to the public.
More generally, HIPAA allows the release of information without the patient's authorization when, in the medical care providers' best judgment, it is in the patient's interest. Despite this language, medical care providers are very reluctant to release information unless it is clearly allowed by HIPAA.