Alaska Application for Family Medical Leave of Absence
Description


How to fill out Application For Family Medical Leave Of Absence?
You can dedicate multiple hours online trying to locate the legal document template that meets the state and federal requirements you need.
US Legal Forms offers a vast array of legal templates that have been reviewed by professionals.
You can conveniently obtain or print the Alaska Application for Family Medical Leave of Absence from your service.
Consult the form description to ensure you have chosen the correct document. If available, utilize the Preview button to review the document template as well.
- If you already possess a US Legal Forms account, you may sign in and then click the Download button.
- Subsequently, you may complete, modify, print, or sign the Alaska Application for Family Medical Leave of Absence.
- Every legal document template you purchase is yours indefinitely.
- To retrieve an additional copy of any purchased form, navigate to the My documents tab and click the corresponding button.
- If you are using the US Legal Forms website for the first time, follow the straightforward instructions below.
- First, ensure you have selected the correct document template for the state/city of your choice.
Form popularity
FAQ
The Alaska Family Leave Act (AFLA) provides a job-protected absence for up to 18 weeks in a 24-month period to eligible employees for a qualifying serious medical condition. It also provides a job-protected absence for up to 18 weeks in a 12-month period to eligible employees for pregnancy, childbirth or adoption.
The Alaska Family Leave Act (AFLA) provides a job-protected absence for up to 18 weeks in a 24-month period to eligible employees for a qualifying serious medical condition. It also provides a job-protected absence for up to 18 weeks in a 12-month period to eligible employees for pregnancy, childbirth or adoption.
Some common reasons employees take a leave of absence are to recover from a serious illness, undergo a medical procedure, assist a family member, take an extended trip or welcome a new child into the family.
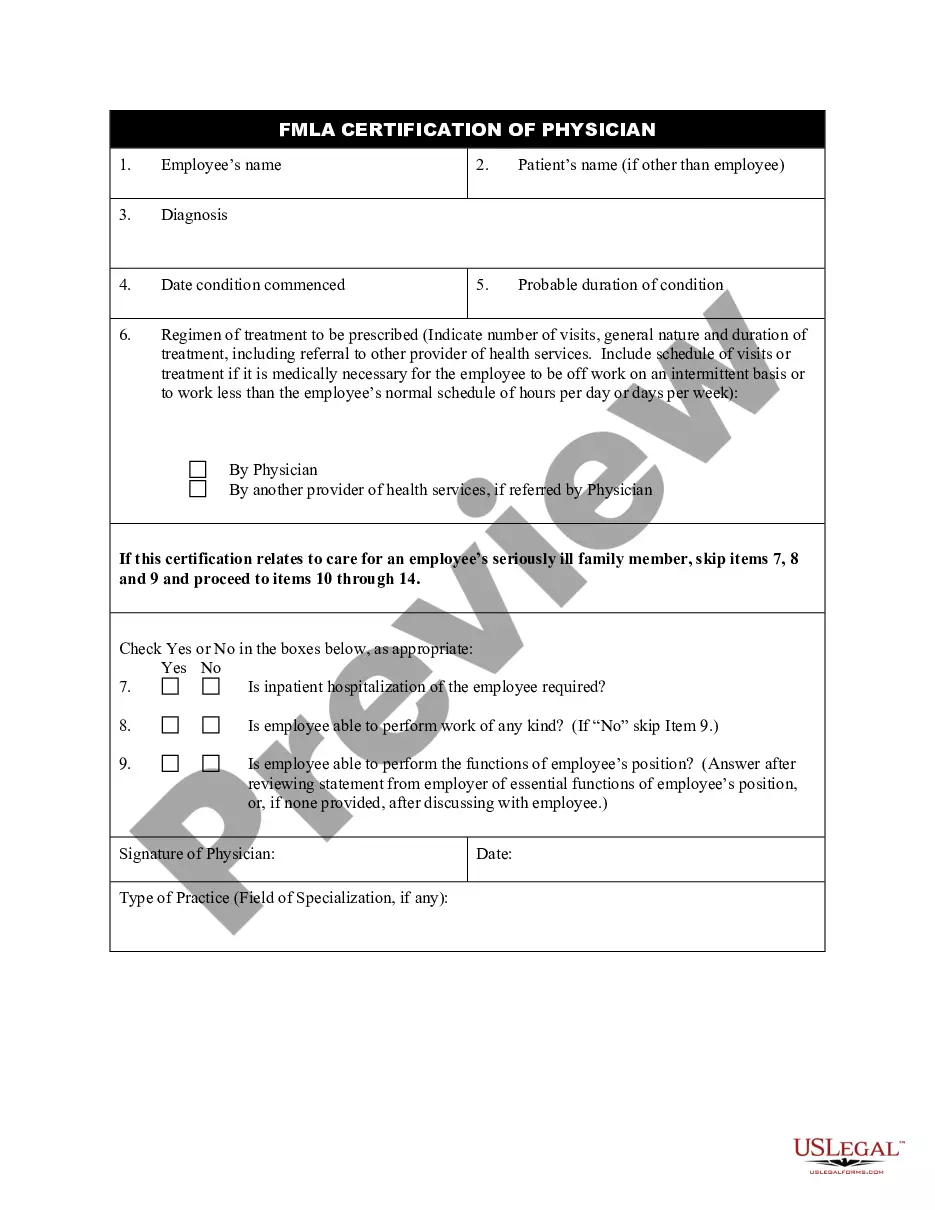
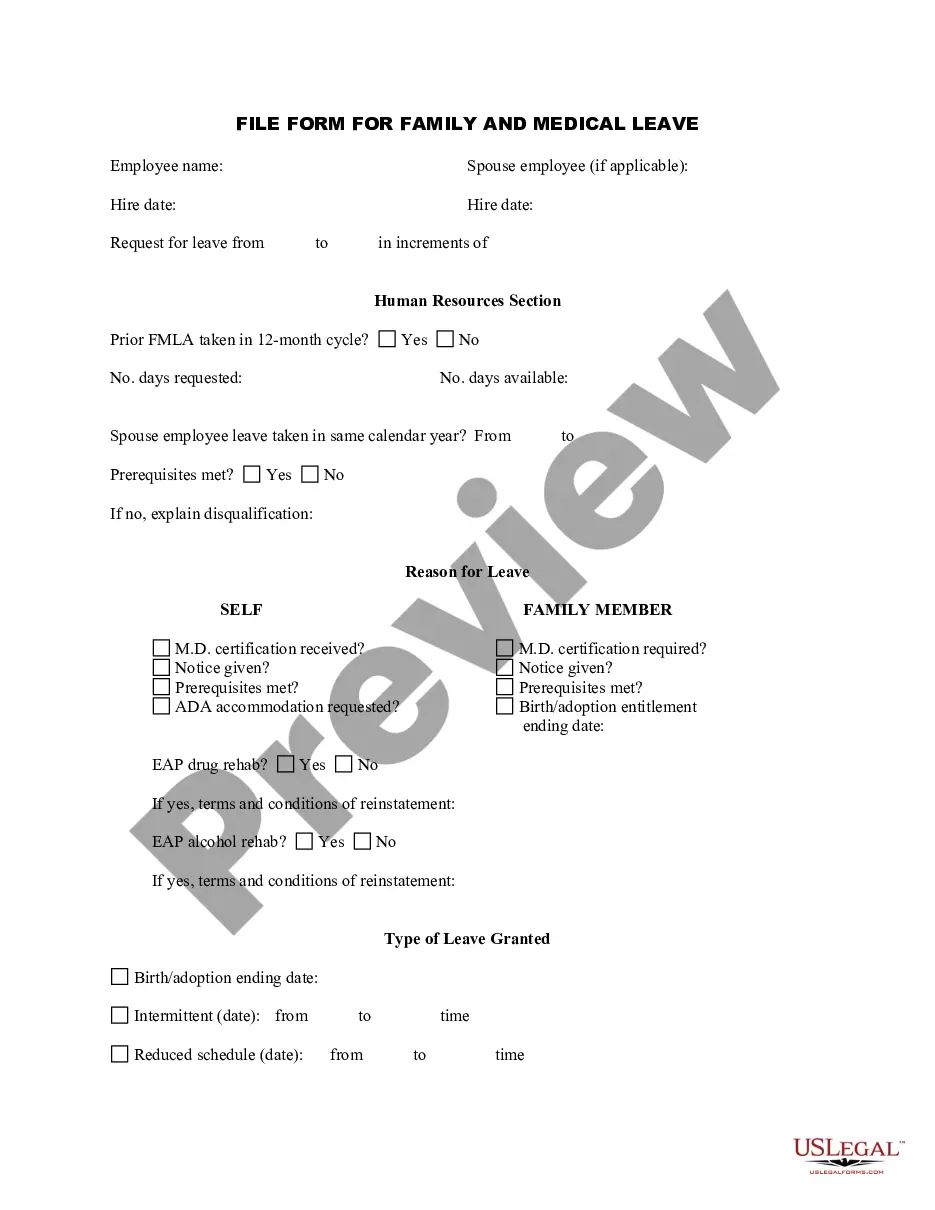
THE FAMILY AND MEDICAL LEAVE ACT (FMLA) requires covered employers to provide up to 12 weeks in a 12 month period of paid or unpaid, job-protected leave to eligible employees for qualifying family and medical reasons (the State of Alaska is a covered employer).
Here's how to ask for a leave of absence from your job:Understand your legal rights regarding time off and pay.Make the request in person.Give sufficient advance notice.If possible, work with your boss to develop an agreeable plan.Keep track of relevant paperwork.
Sample LetterI am writing to inform you that I will be taking a sick leave because of a serious infection in my throat. I will be absent from work until October 14. I have attached a note from my doctor to confirm that it is necessary for my health and the health of my coworkers for me to take a medical leave.
FMLA leave is unpaid leave. However, workers may choose to, or employers may require them to, substitute accrued paid sick, vacation, or personal time for FMLA leave. Substitute means that the paid leave provided by the employer will run concurrently with the unpaid FMLA leave.
Please be advised that I hereby request an FMLA leave for a period of (number of weeks) in connection with my serious health condition. The leave is to start on (date). Attached is my medical note reflecting the need for FMLA leave. Please let me know whether you approve this leave at your earliest convenience.
Your request for a leave of absenceDuring the first paragraph of your letter, state your request for a leave of absence. This is where you include the start date of your absence and the approximate return date. You can include your reason for a leave of absence with as much detail as you feel comfortable with.
Leave and Reinstatement Rights Employees are entitled to continue their health insurance while on leave, at the same cost they must pay while working. FMLA leave is unpaid.