Alaska Family and Medical Leave Request Form
Description




How to fill out Family And Medical Leave Request Form?
US Legal Forms - one of the largest collections of legal documents in the United States - offers a variety of legal document templates that you can download or print. By utilizing the site, you can access thousands of forms for business and personal use, classified by categories, states, or keywords.
You can obtain the most recent versions of forms, like the Alaska Family and Medical Leave Request Form, in just a few seconds. If you already have a monthly membership, Log In to access the Alaska Family and Medical Leave Request Form from your US Legal Forms library. The Download button will appear on every form you view. You can access all previously obtained forms from the My documents section of your account.
If you are using US Legal Forms for the first time, here are simple steps to get started: Make sure you have chosen the correct form for your city/state. Click the Review button to check the form`s details. Review the form information to ensure you have selected the right form.
Every template you add to your account has no expiration date and is yours indefinitely. So, if you wish to download or print another copy, just visit the My documents section and click on the form you need.
Access the Alaska Family and Medical Leave Request Form with US Legal Forms, the most extensive collection of legal document templates. Utilize thousands of professional and state-specific templates that fulfill your business or personal needs and requirements.
- If the form does not meet your needs, utilize the Search field at the top of the screen to find one that does.
- If you are satisfied with the form, confirm your choice by clicking the Purchase now button.
- Then, select your preferred pricing plan and provide your credentials to register for an account.
- Complete the transaction. Use a credit card or PayPal account to finish the transaction.
- Select the format and download the form to your device.
- Edit. Fill out, modify, and print and sign the obtained Alaska Family and Medical Leave Request Form.
Form popularity
FAQ
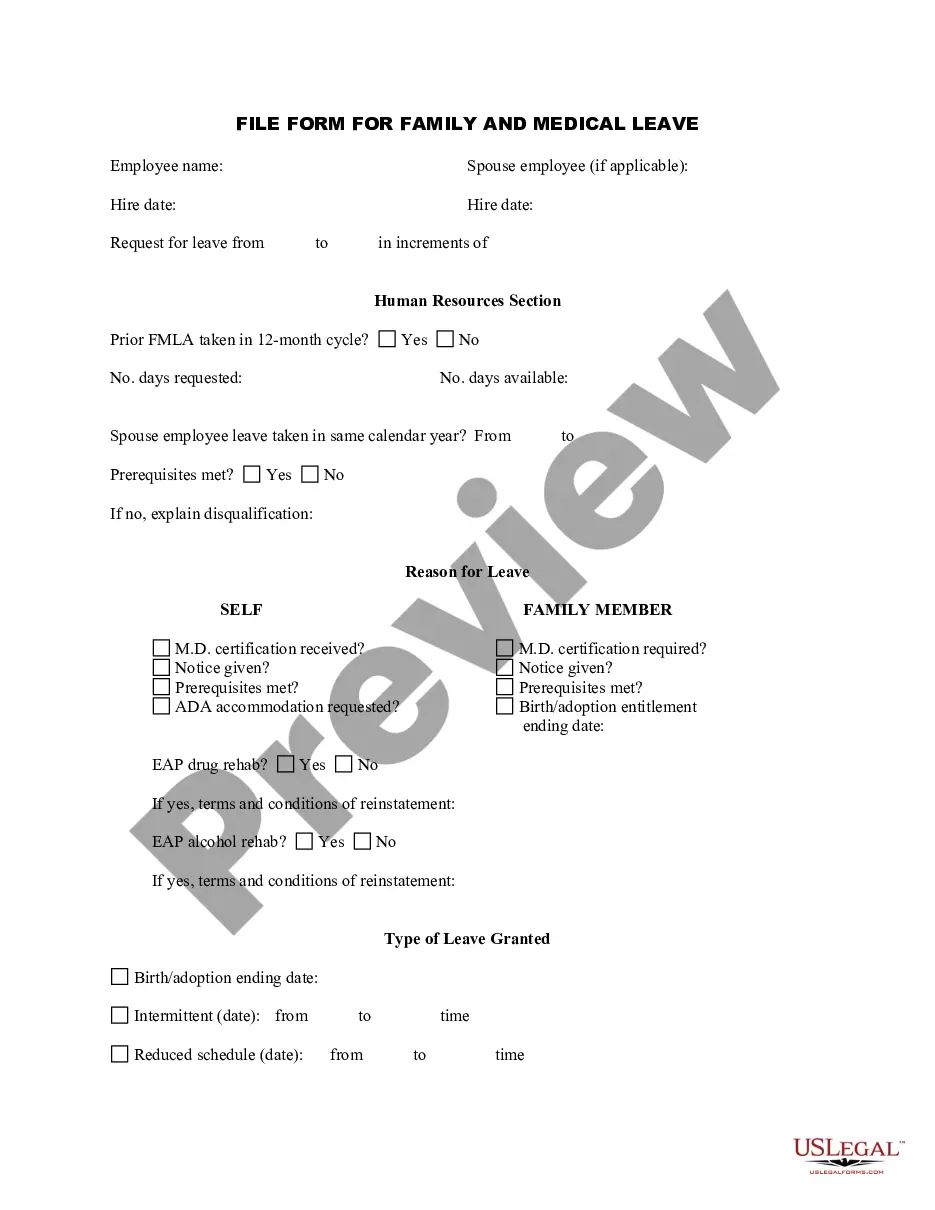
The Alaska Family Leave Act (AFLA) provides a job-protected absence for up to 18 weeks in a 24-month period to eligible employees for a qualifying serious medical condition. It also provides a job-protected absence for up to 18 weeks in a 12-month period to eligible employees for pregnancy, childbirth or adoption.
Include a brief explanation of why you are taking the leave and perhaps state where you will be while you are away. If it is possible, offer your assistance and provide the best way to contact you during your time off. Be sure to thank your employer for considering your request.
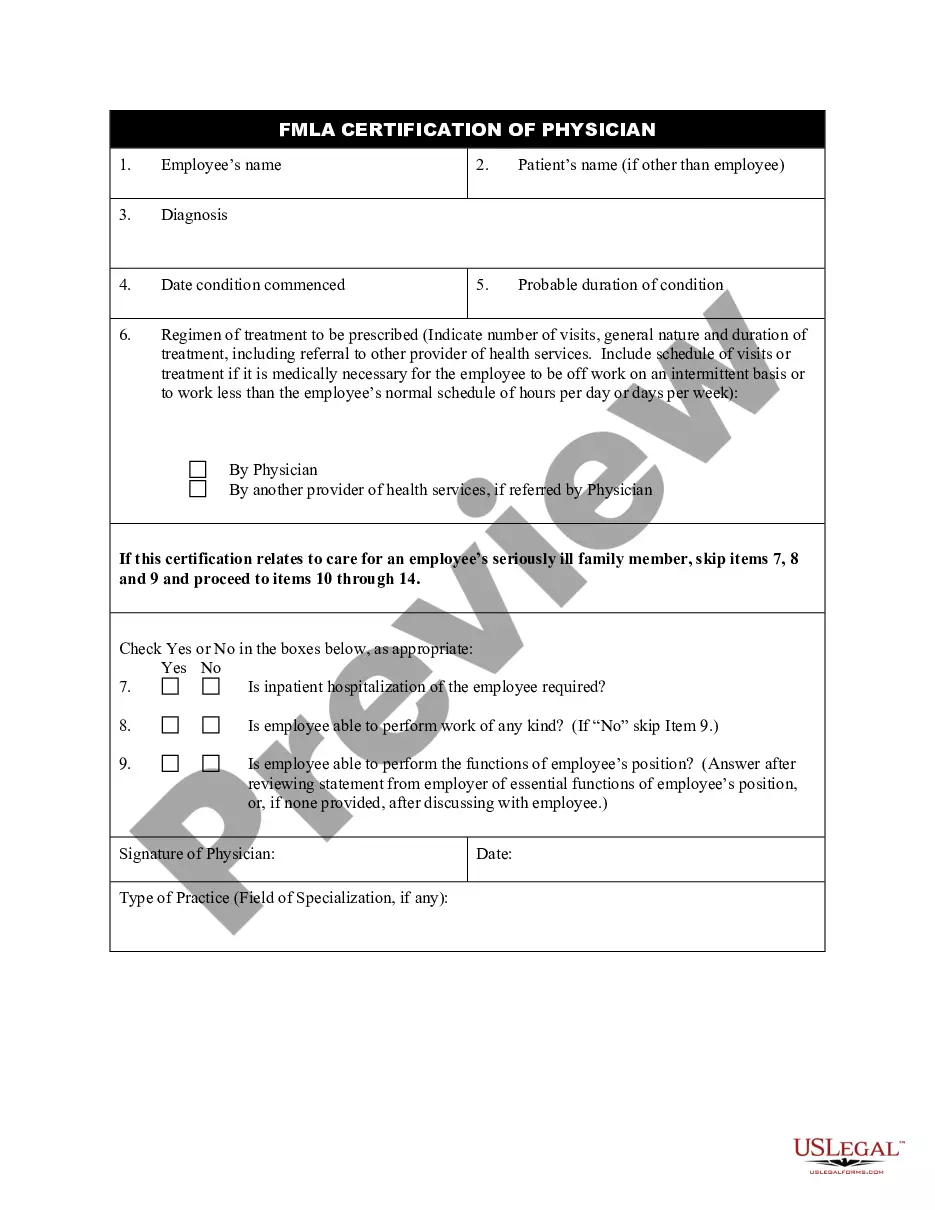
Dear (Supervisor / HR Manager): Please be advised that I hereby request an FMLA leave for a period of (number of weeks) in connection with my serious health condition. The leave is to start on (date). Attached is my medical note reflecting the need for FMLA leave.
I will be having surgerymy surgeon has ordered a minimum three-week recovery period (see doctor's signed recommendation attached.) I am happy to assist in handling any necessary preparations before beginning my leave, including training colleagues on upcoming projects. Thank you so much for your understanding.
I am writing to inform you that I will be taking a sick leave because of a serious infection in my throat. I will be absent from work until October 14. I have attached a note from my doctor to confirm that it is necessary for my health and the health of my coworkers for me to take a medical leave.
FMLA leave is unpaid leave. However, workers may choose to, or employers may require them to, substitute accrued paid sick, vacation, or personal time for FMLA leave. Substitute means that the paid leave provided by the employer will run concurrently with the unpaid FMLA leave.
Leave and Reinstatement Rights Employees are entitled to continue their health insurance while on leave, at the same cost they must pay while working. FMLA leave is unpaid.
THE FAMILY AND MEDICAL LEAVE ACT (FMLA) requires covered employers to provide up to 12 weeks in a 12 month period of paid or unpaid, job-protected leave to eligible employees for qualifying family and medical reasons (the State of Alaska is a covered employer).
Your request for a leave of absenceDuring the first paragraph of your letter, state your request for a leave of absence. This is where you include the start date of your absence and the approximate return date. You can include your reason for a leave of absence with as much detail as you feel comfortable with.