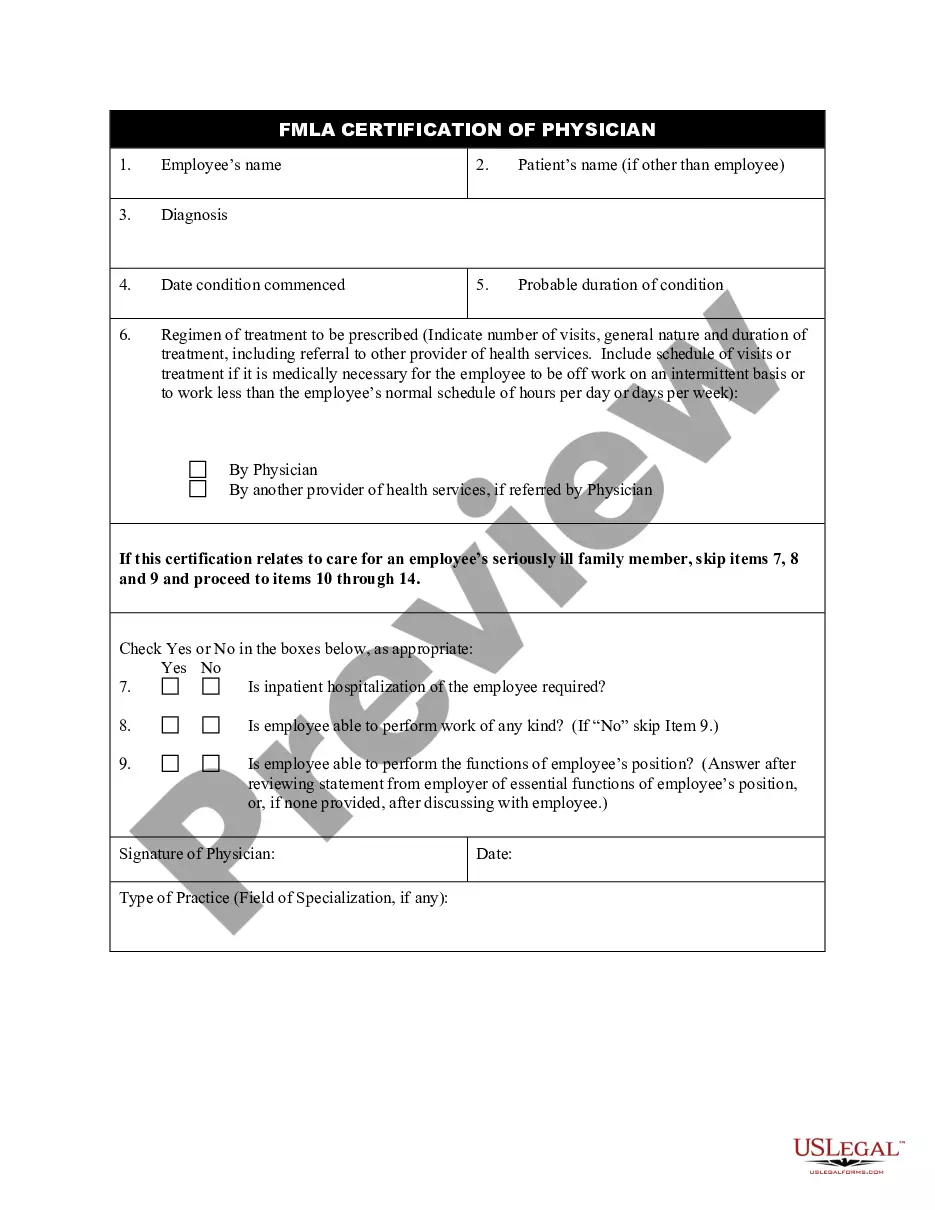
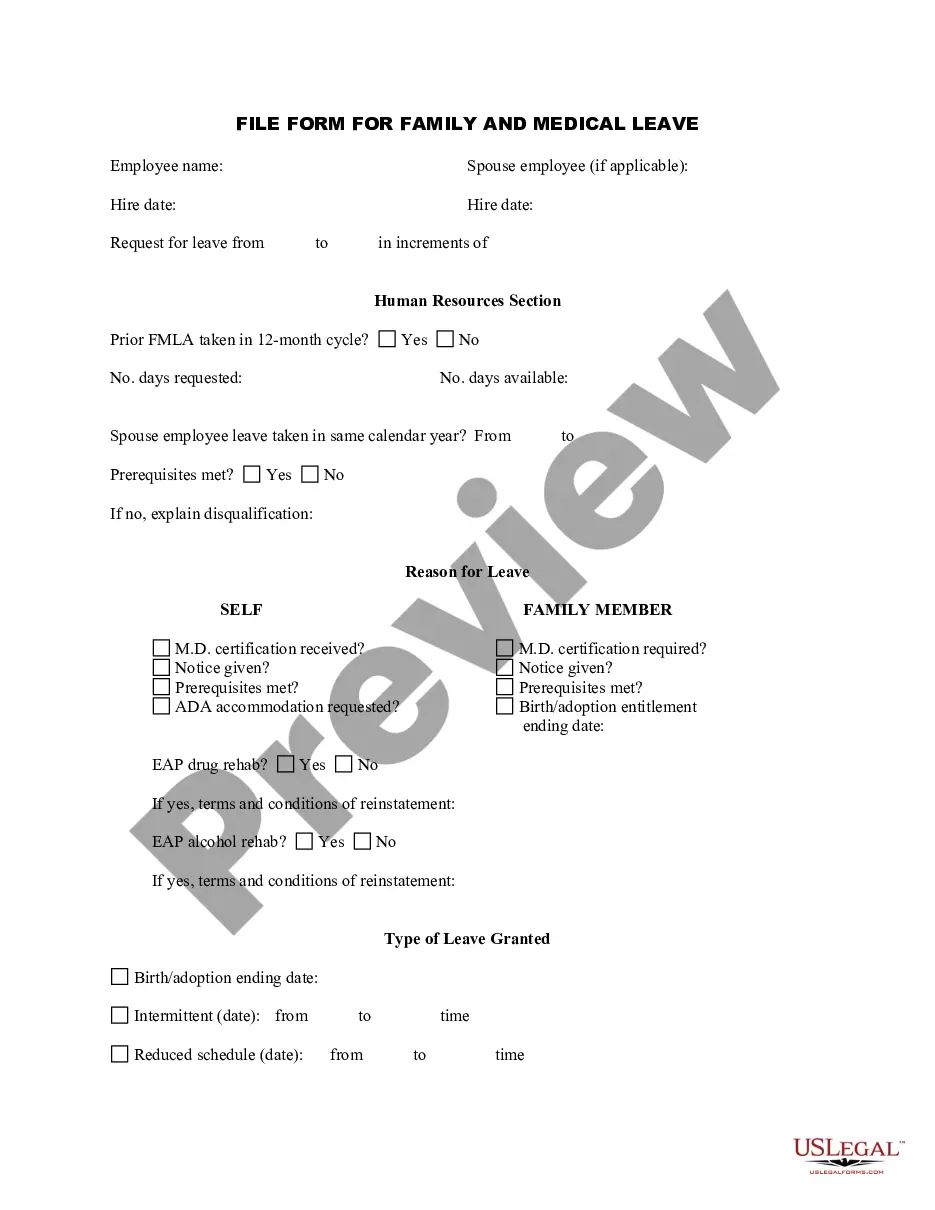
This form is an application for Family and Medical Leave. It is to be filled out by an employee who is requesting a leave of absence.
Travis Texas Employee Application for FMLA
State:
Multi-State
County:
Travis
Control #:
US-AHI-200
Format:
Word;
Rich Text
Instant download
Description
Free preview


How to fill out Employee Application For FMLA?
Creating documents for business or individual requests is always a significant responsibility.
When formulating a contract, a governmental service request, or a power of attorney, it’s crucial to consider all federal and state regulations and laws of the specific area.
Nevertheless, smaller counties and even municipal areas also have legislative requirements that you need to keep in mind.
Make sure the template meets legal requirements and click Buy Now. Select the subscription option, then Log In or create an account with US Legal Forms. Use your credit card or PayPal to pay for your subscription. Download the chosen document in your desired format, print it, or fill it out electronically. A remarkable feature of the US Legal Forms library is that all the documents you have purchased remain accessible - you can retrieve them in your profile under the My documents tab at any time. Join the platform and swiftly obtain verified legal forms for any circumstance with just a few clicks!
- All these factors make it challenging and time-consuming to prepare the Travis Employee Application for FMLA without professional help.
- It's straightforward to prevent unnecessary expenditures on lawyers drafting your documents and to create a legally binding Travis Employee Application for FMLA independently, utilizing the US Legal Forms online database.
- It represents the largest online repository of state-specific legal documents that have been professionally verified, so you can trust their authenticity when selecting a template for your region.
- Users with prior subscriptions only need to Log In to their accounts to retrieve the necessary form.
- If you still lack a subscription, follow the step-by-step instructions below to acquire the Travis Employee Application for FMLA.
- Browse the page you've opened and verify if it contains the document you need.
- To do this, utilize the form description and preview if these features are available.
Form popularity
FAQ
FMLA Form WH-380-F for Family Health Condition You'll need to provide your family member's name and your relationship to that family member (only certain relatives qualify). You'll also need to describe the type of care you must provide and how much time off you will need.
Dear (Supervisor / HR Manager): Please be advised that I hereby request an FMLA leave for a period of (number of weeks) in connection with my serious health condition. The leave is to start on (date). Attached is my medical note reflecting the need for FMLA leave.
FMLA certification is a medical confirmation that is generally required for employees to take leave per the Family Medical Leave Act. Generally, this is required in the case of employees or their direct family members sustaining a serious health condition that requires time off work for caregiving or recuperation.
You may receive up to 8 weeks of Paid Family Leave (PFL) benefits in a 12 month period. The daily benefit amount is calculated by dividing your weekly benefit amount by seven.
Dear (Supervisor / HR Manager): Please be advised that I hereby request an FMLA leave for a period of (number of weeks) in connection with my serious health condition. The leave is to start on (date). Attached is my medical note reflecting the need for FMLA leave.
Though the FMLA itself is unpaid, it is sometimes possible under certain specific circumstances to use paid leave that you've accrued on the job as a way to get paid during your FMLA leave. The types of paid leave that might be considered include vacation days and sick days, as well as other types of paid leave.
When requesting a formal leave of absence, your letter should include: Request for a leave of absence, The dates you expect to be away from work, The date you plan to return to work, An offer to provide assistance, if feasible, Thanks for considering your request.
While FMLA guarantees the employee unpaid leave of 12 weeks over a 12 month period, the PFL provides for up to 6 weeks of paid leave in a 12 month period. 4. While the PFL does provide for partial pay during leave, however, it does not guarantee leave.
In order to be eligible to take leave under the FMLA, an employee must (1) work for a covered employer, (2) work 1,250 hours during the 12 months prior to the start of leave, (3) work at a location where 50 or more employees work at that location or within 75 miles of it, and (4) have worked for the employer for 12
Dear name, I am writing this letter to inform you that I need to take sick leave from work. I will need to remain off work until date. I've included a letter from my doctor to confirm that I need to take that amount of time off to fully recover.