Wisconsin Release and Authorization
Overview of this form
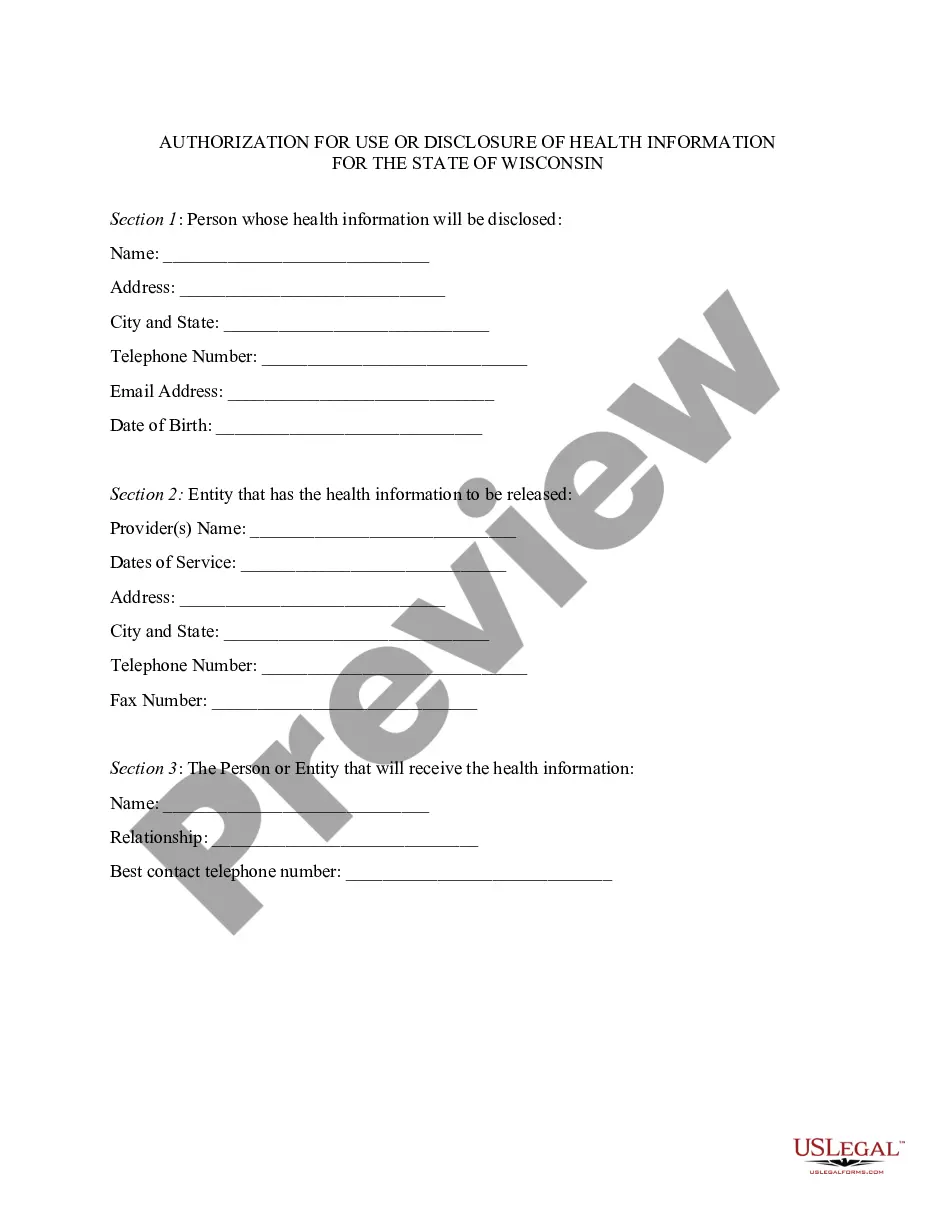
The Wisconsin Release and Authorization is a HIPAA authorization form specifically tailored for residents of Wisconsin. This form allows individuals to authorize their health care providers to use and disclose their protected health information to designated persons. Unlike general authorization forms, this version adheres to the specific requirements outlined in Wisconsin law, making it a crucial tool for managing personal medical information securely.
What’s included in this form
- Authorization statement for health care providers to disclose medical information.
- Effective period covering all past, present, and future health care.
- Extent of authorization to release complete health records.
- Purpose for which the information may be used.
- Patient information section including name, address, and contact details.
- Signature and date fields to validate the authorization.



When to use this document
This form should be used whenever a patient wishes to grant permission for their health care provider to share their protected health information with another person or entity. It is essential in situations where family members, insurance companies, or other healthcare professionals need access to the medical records for treatment, billing, or consultation purposes.
Intended users of this form
- Patients in Wisconsin planning to share their medical information with others.
- Family members acting on behalf of a patient to manage health-related matters.
- Healthcare providers who require official authorization to disclose patient information.
- Legal representatives of patients needing access to medical records for legal purposes.
How to prepare this document
- Identify and enter the name and contact information of your health care provider.
- Provide the name of the individual you authorize to receive your health information.
- Fill in your personal information, including your name, address, and date of birth.
- Read and understand the terms of the authorization, including the extent of information covered.
- Sign and date the form to validate the release of your information.
Notarization guidance
This form does not typically require notarization unless specified by local law. However, it is recommended to check if any particular circumstances may necessitate notarization.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Avoid these common issues
- Failing to specify the recipient of the health information.
- Not providing complete personal information, leading to processing delays.
- Overlooking the expiration terms of the authorization.
- Neglecting to sign and date the form, which invalidates the authorization.
Advantages of online completion
- Easy download and immediate access to the form in a convenient format.
- Editability allows for quick adjustments to tailor the form to your specific needs.
- Reliability ensured by using a form drafted by licensed attorneys familiar with Wisconsin law.
Looking for another form?
Form popularity
FAQ
A HIPAA authorization form, also known as a HIPAA release form, is a document that individual signs for their health provider before the entity may use or disclose their protected health information (PHI).
By setting up a Release Authorization (ARI), you are giving customer service your permission to disclose information about your accounts to another person. Typically, this is used to give account access to a spouse or other family member.
I understand that this information is protected by law and cannot be released/requested without my written consent unless otherwise provided by law. I further understand that this consent may be revoked by me, in writing at any time, except if the information has already been released or obtained.
The medical record information release (HIPAA) form allows a patient to give authorization to a 3rd party and access their health records.
Description. The Third Party Authorization form authorizes a person other than the payor or recipient to act on the payor's or recipient's behalf. A Family Responsibility Office (FRO) support payor or support recipient may designate this person to request and receive information from the FRO regarding their case.