Washington Provider Payment Account Change Form is a document used to update and maintain payment information for providers in the Washington State Health Care Authority (HCA). This form is used to update the payment account information in the HCA's provider payment system. It enables providers to update their banking information, change the payment method (e.g. direct deposit or check), or make other changes to their payment account information. There are two types of Washington Provider Payment Account Change Form: one for providers registered with the HCA and one for providers not registered with the HCA. Both forms must be filled out and submitted electronically to the HCA in order to make changes to the provider's payment account information.
Washington Provider Payment Account Change Form
Description
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Looking for another form?
How to fill out Washington Provider Payment Account Change Form?
US Legal Forms is the most easy and cost-effective way to locate appropriate legal templates. It’s the most extensive online library of business and personal legal documentation drafted and checked by lawyers. Here, you can find printable and fillable blanks that comply with national and local laws - just like your Washington Provider Payment Account Change Form.
Getting your template requires only a few simple steps. Users that already have an account with a valid subscription only need to log in to the website and download the document on their device. Later, they can find it in their profile in the My Forms tab.
And here’s how you can get a professionally drafted Washington Provider Payment Account Change Form if you are using US Legal Forms for the first time:
- Read the form description or preview the document to make certain you’ve found the one corresponding to your needs, or find another one using the search tab above.
- Click Buy now when you’re sure of its compatibility with all the requirements, and choose the subscription plan you prefer most.
- Create an account with our service, sign in, and purchase your subscription using PayPal or you credit card.
- Choose the preferred file format for your Washington Provider Payment Account Change Form and save it on your device with the appropriate button.
Once you save a template, you can reaccess it whenever you want - simply find it in your profile, re-download it for printing and manual completion or import it to an online editor to fill it out and sign more effectively.
Take full advantage of US Legal Forms, your reliable assistant in obtaining the corresponding formal paperwork. Try it out!
Form popularity
FAQ
Please use CHPW's Payer Identifier: CHPWA.
Medical Bills must be filed within 12 months of the date of service for all services rendered in Washington.
Submit Claims to Molina through your EDI clearinghouse using Payer ID 38336, refer to our website .molinahealthcare.com/providers/common/medicaid/ediera/edi/benefits.aspx for additional information.
ProviderOne is the computer system that coordinates with the health plans. It also sends you letters and handbooks. The number on the card is your ProviderOne client number.
Apple Health is the name for Medicaid in Washington.
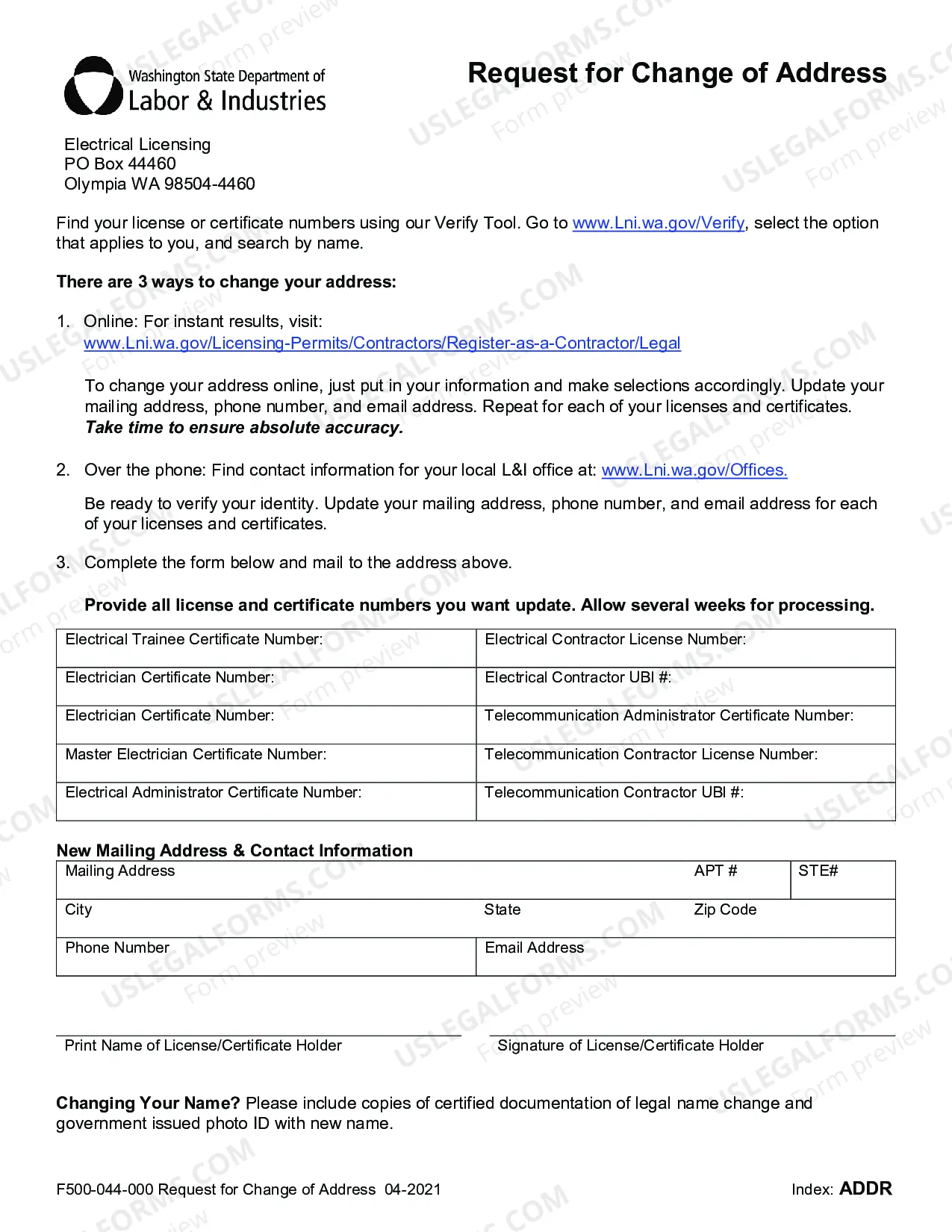
Go to .Lni.wa.gov/Verify, select the option that applies to you, and search by name. To change your address online, just put in your information and make selections ingly. Update your mailing address, phone number, and email address. Repeat for each of your licenses and certificates.
Select ClaimRemedi, Billing Agent/Clearinghouse ProviderOne ID: 2010950.