Delaware Release and Authorization
Understanding this form
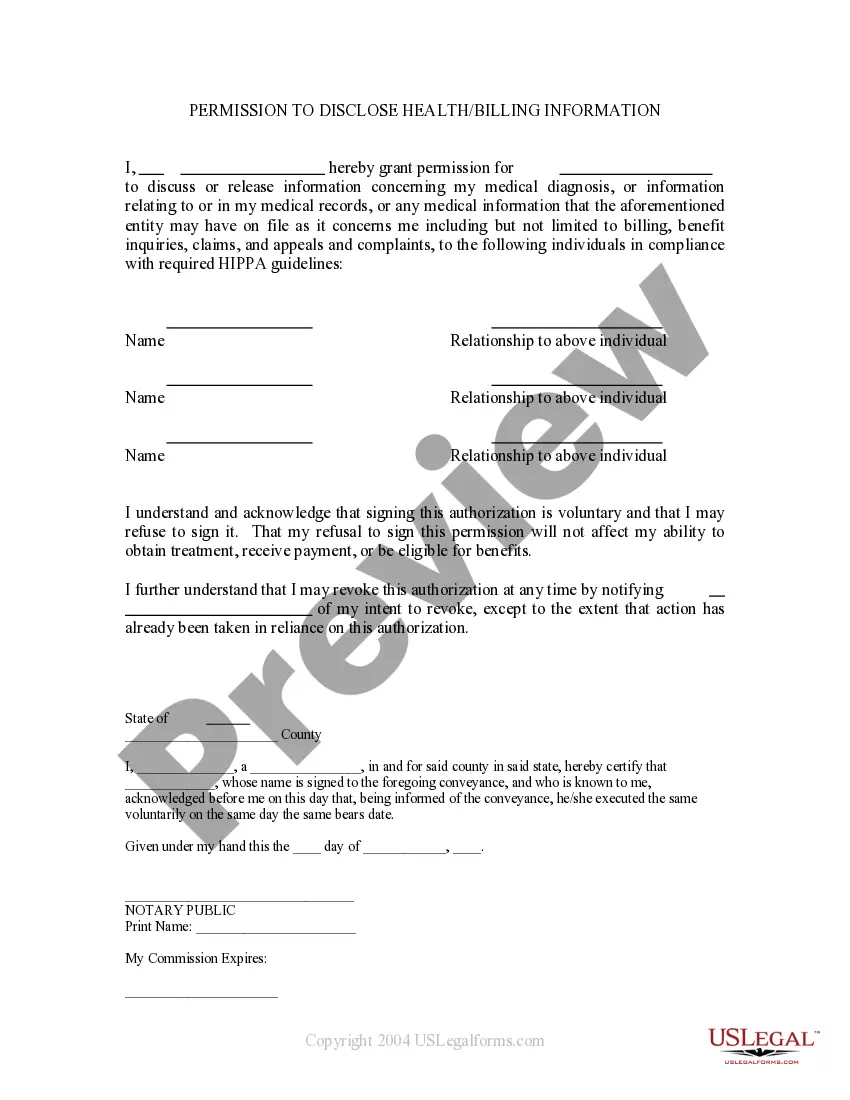
The Delaware Release and Authorization form is a HIPAA authorization document specifically designed for residents of Delaware. This form allows individuals to authorize their healthcare providers to use and disclose their protected health information to designated parties. It is essential for ensuring that personal health information can be shared legally for treatment, billing, or other purposes. What sets this form apart from other authorization forms is its compliance with Delaware laws and its specific provisions regarding the disclosure of medical information.
Main sections of this form
- Authorization statement for use or disclosure of protected health information.
- Identification of the healthcare provider and the individual authorized to receive information.
- Effective period covering all past, present, and future healthcare.
- Extent of authorization, including complete health records.
- Revocation rights allowing the patient to revoke authorization at any time.
- Understanding of disclosure limitations, as the recipient may further disclose the information.



When this form is needed
This form should be used when a patient needs to provide permission for their healthcare provider to share their medical information with another individual or entity. Common scenarios include situations where a patient wants a family member to have access to their medical records during treatment, or when a patient needs to authorize billing or claims processing by an insurance company.
Who can use this document
- Patients seeking to share their medical information with healthcare providers or family members.
- Legal representatives of patients who need to authorize information disclosures on their behalf.
- Individuals requiring access to someone else's health information for treatment or coordination of care.
How to complete this form
- Identify the healthcare provider by filling in their name, title or facility, address, and telephone number.
- Specify the individual authorized to receive the protected health information.
- Complete patient information including name, address, phone number, email address, and date of birth.
- Sign and date the authorization to validate the request for disclosure.
- Understand your rights regarding revocation of this authorization at any time.
Notarization guidance
This form does not typically require notarization unless specified by local law. Ensure to check any specific state requirements that may necessitate notarization for additional legal protection.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Typical mistakes to avoid
- Failing to provide full and accurate identification of the healthcare provider.
- Leaving the effective period section incomplete, which can cause confusion regarding the duration of authorization.
- Not signing or dating the form, rendering it invalid.
- Assuming that the authorization can be revoked verbally; it must be done in writing.
Why complete this form online
- Convenience of downloading and completing the form at your own pace.
- Editability allows you to personalize the form based on your specific needs.
- Access to reliable legal templates drafted by licensed attorneys ensures compliance and validity.
Looking for another form?
Form popularity
FAQ
Writing an authorization to release information requires a clear structure. Begin with a title, such as 'Authorization to Release Information,' and include the names and descriptors of all parties involved. Provide a detailed description of the information to be released and specify its purpose. After ensuring all required elements are present, sign and date the document, confirming your agreement to the Delaware Release and Authorization.
To successfully fill out an authorization form, start by clearly identifying the parties involved and the information to be disclosed. Specify the purpose of the information release and the duration for which the authorization remains valid. Finally, remember to sign and date the form, affirming your consent to the release. If you need support, our USLegalForms platform offers step-by-step guidance.
In Delaware, the relevant tax form for a power of attorney is typically Form 8879, which allows someone to file tax returns on behalf of another. It is important to check the specific requirements as they pertain to the Delaware Release and Authorization. Additionally, you can access templates and guidance on our platform, USLegalForms, to simplify your process.
A patient authorization form for a Delaware Release and Authorization must include the patient's full name, date of birth, and contact information. Clearly state the specific information being released, along with the name of the entity that will receive the information. The form should also outline the purpose of the disclosure and include the patient's signature and date, ensuring legal compliance.
Filling out a Delaware Release and Authorization form involves gathering all necessary personal details, such as names and contact information. Begin by providing the specifics of the information you wish to release and identifying who should receive it. Ensure to sign the authorization at the bottom, confirming your consent clearly. For an easy process, consider using our platform, USLegalForms, which offers guided assistance.
To create a valid Delaware Release and Authorization, ensure the document includes the name and contact information of the individual or facility providing the information. Additionally, clearly identify the person or organization receiving the information. Include a detailed description of the information to be released, specify the purpose for its release, and state the duration of the authorization. Lastly, the individual must sign and date the form, affirming their consent.
An authorization of release refers to the official act of permitting the sharing of personal data with designated parties. This authorization ensures that individuals understand what information is being disclosed and for what purposes. In the scope of the Delaware Release and Authorization, this document establishes accountability and protects personal privacy. By using uslegalforms, you can simplify the creation of an authorization of release, tailoring it to suit your specific requirements.
An authorization to release information is typically valid for a specified period, often stated within the document itself. Most authorization forms outline the duration for which the consent remains in effect, commonly ranging from a few months to several years. In the case of Delaware Release and Authorization, it's essential to note any expiration dates to ensure compliance. With uslegalforms, you can easily manage and update your authorization timelines as needed.
The purpose of an authorization form is to provide lawful consent for the release and sharing of personal information. This form is crucial for protecting privacy rights and ensuring individuals have control over their data. Within the Delaware Release and Authorization context, the form outlines the scope and limitations of the information that can be shared. By utilizing services from uslegalforms, you can create an effective authorization form that fulfills all legal requirements.
An authorization release is a formal document that grants permission to disclose an individual's private information to specified parties. It serves as a safeguard for both the requester and the person being evaluated, ensuring transparency and trust. In relation to the Delaware Release and Authorization, this document clearly outlines what information can be shared and with whom. You can rely on uslegalforms to provide you with template forms that meet your needs for an authorization release.