Santa Clara California Authorization for Use and / or Disclosure of Protected Health Information
Description






How to fill out Authorization For Use And / Or Disclosure Of Protected Health Information?
Generating legal documents is essential in contemporary society.
However, it is not always necessary to obtain expert assistance to create certain documents from scratch, like the Santa Clara Authorization for Use and/or Disclosure of Protected Health Information, using a service such as US Legal Forms.
US Legal Forms offers more than 85,000 templates across different categories, including living wills, real estate documents, and divorce forms. All templates are categorized according to their respective state, simplifying the search process.
If you're already a US Legal Forms subscriber, you can find the necessary Santa Clara Authorization for Use and/or Disclosure of Protected Health Information, Log In to your account, and download it.
It's important to note that our platform cannot entirely replace a lawyer. If you are faced with a particularly complex issue, we advise consulting an attorney to review your form before executing and submitting it.
- Review the document's preview and outline (if present) to acquire an overall understanding of what you will receive upon downloading the template.
- Make sure that the template you select pertains specifically to your state/county/region since local laws can affect the validity of particular records.
- Look at similar documents or restart your search to find the correct file.
- Click Buy now and create your account. If you already have one, opt to Log In.
- Choose the pricing {plan, then select an appropriate payment method, and purchase the Santa Clara Authorization for Use and/or Disclosure of Protected Health Information.
- Decide to download the form template in any available file format.
- Go to the My documents section to re-download the document.
Form popularity
FAQ
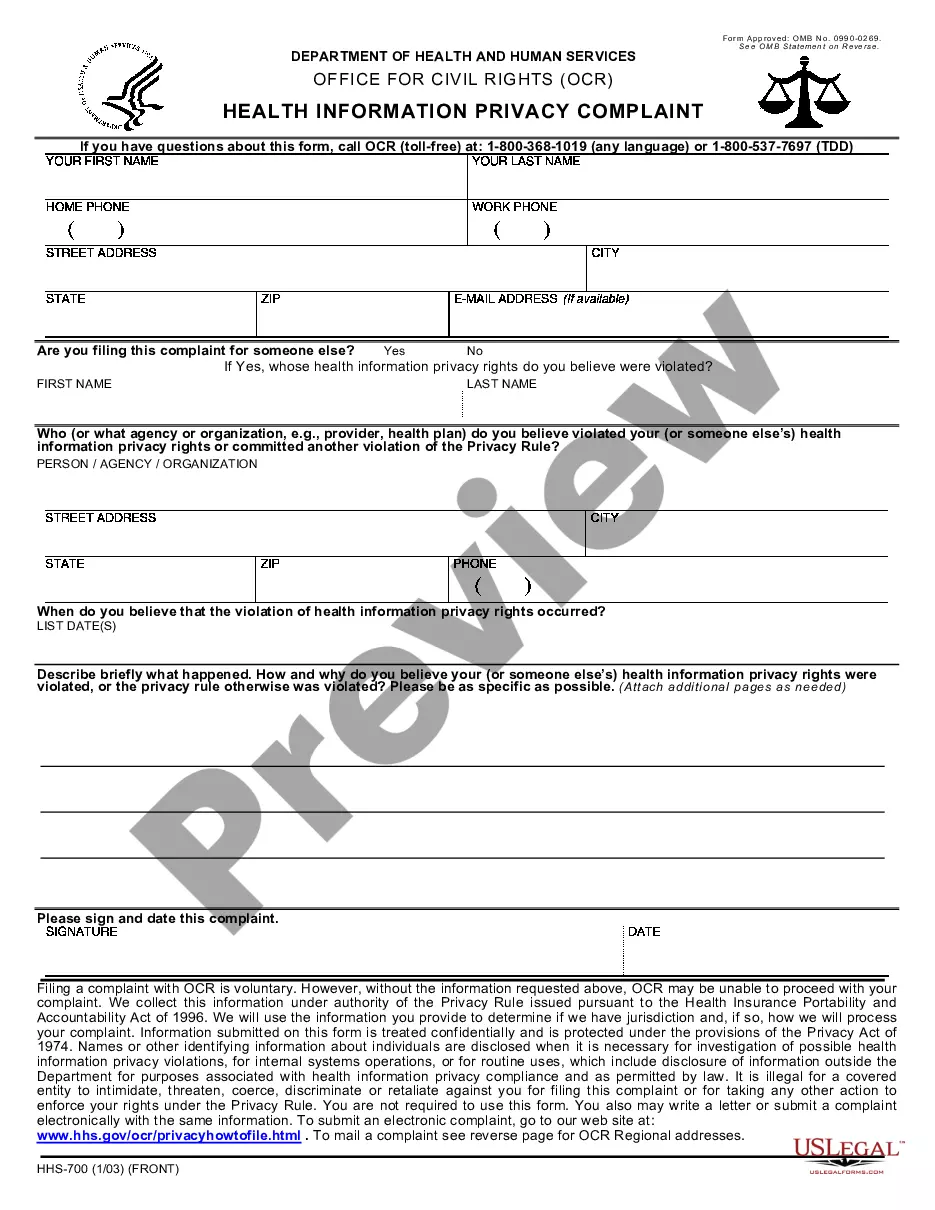
Release of information (ROI) is the process of providing access to protected health information (PHI) to an individual or entity authorized to receive or review it.
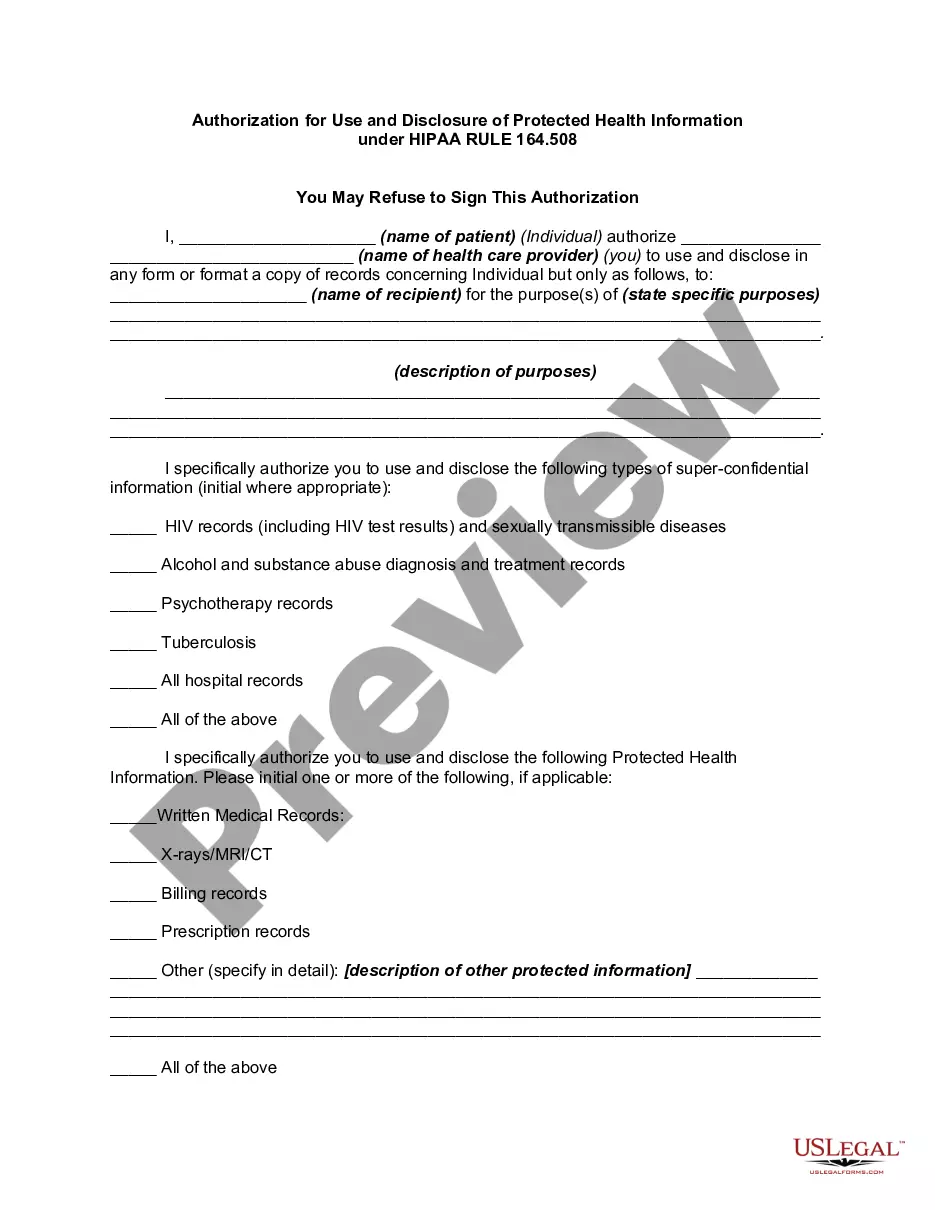
Valid HIPAA Authorizations: A Checklist No Compound Authorizations. The authorization may not be combined with any other document such as a consent for treatment.Core Elements.Required Statements.Marketing or Sale of PHI.Completed in Full.Written in Plain Language.Give the Patient a Copy.Retain the Authorization.
A signature and date that the authorization is signed by an individual or an individual's representative. If a representative is signing the form, the relationship with the patient must be detailed along with a description of the representative's authority to act on behalf of the patient.
The core elements of a valid authorization include: A meaningful description of the information to be disclosed. The name of the individual or the name of the person authorized to make the requested disclosure. The name or other identification of the recipient of the information.
HIPAA does not specify any requirements for a patient's written request to access information, but a good form would typically include: (i) the patient's identifying and contact information; (ii) a specific description of the records requested (including the date range and type of records requested); (iii) the format
This form is used to release your protected health information as required by federal and state privacy laws. Your authorization allows the Health Plan (your health insurance carrier or HMO) to release your protected health information to a person or organization that you choose.
An authorization must specify a number of elements, including a description of the protected health information to be used and disclosed, the person authorized to make the use or disclosure, the person to whom the covered entity may make the disclosure, an expiration date, and, in some cases, the purpose for which the