ADA Questionnaire for Physician
What this document covers
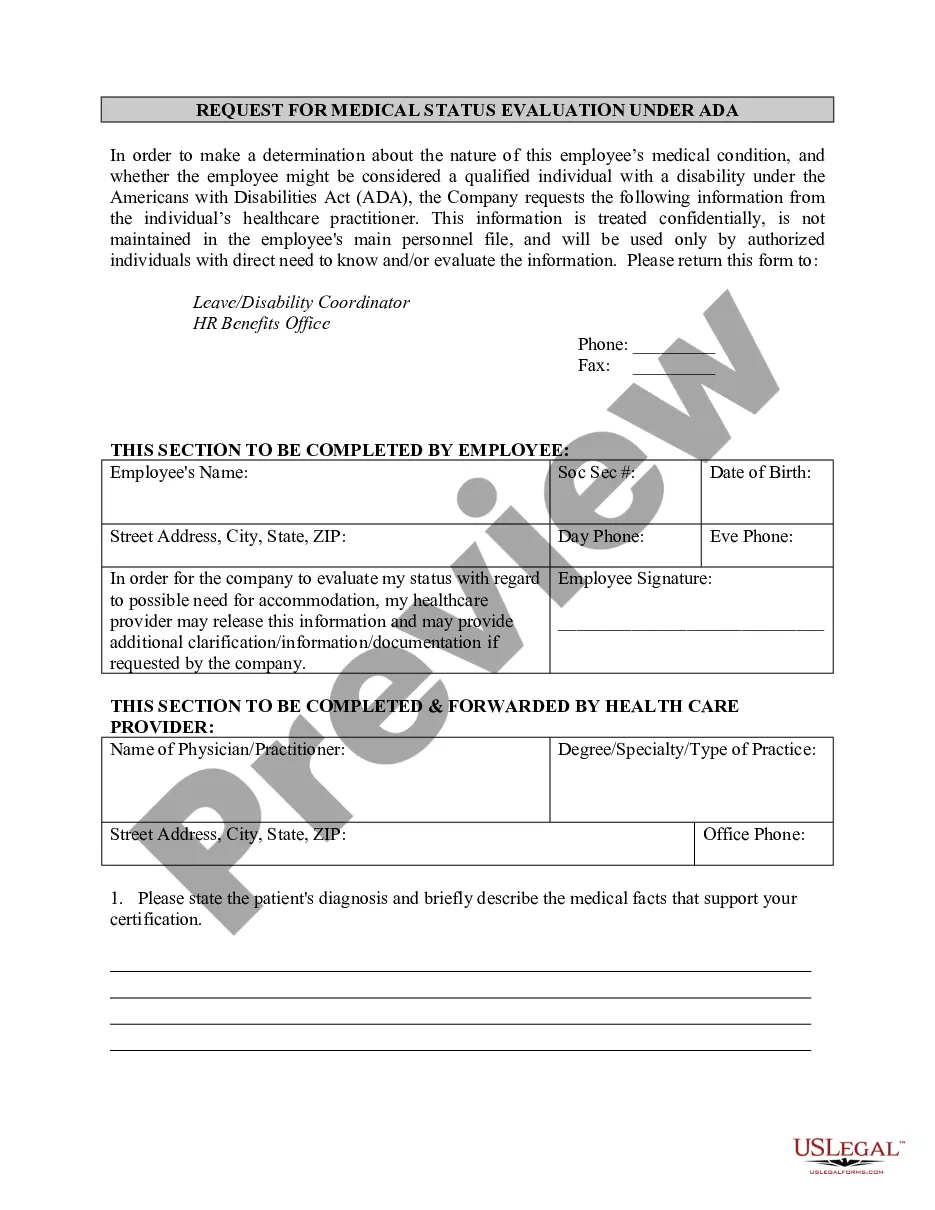
The ADA Questionnaire for Physician is a legal document that enables employers to evaluate whether an employee has a disability as defined by the Americans With Disabilities Act (ADA). This form plays a crucial role in determining necessary accommodations to support the employee's job performance safely and effectively. It differs from other medical inquiries as it specifically focuses on confirming a disability and the potential need for reasonable accommodations in the workplace.
Key parts of this document
- Date and contact information for both the employer and the physician.
- Employee's details including name, position, and a signed release for medical information.
- A clear explanation of the employer's concerns regarding the employee's job performance related to potential disability.
- A questionnaire that guides the physician in providing necessary medical insights.
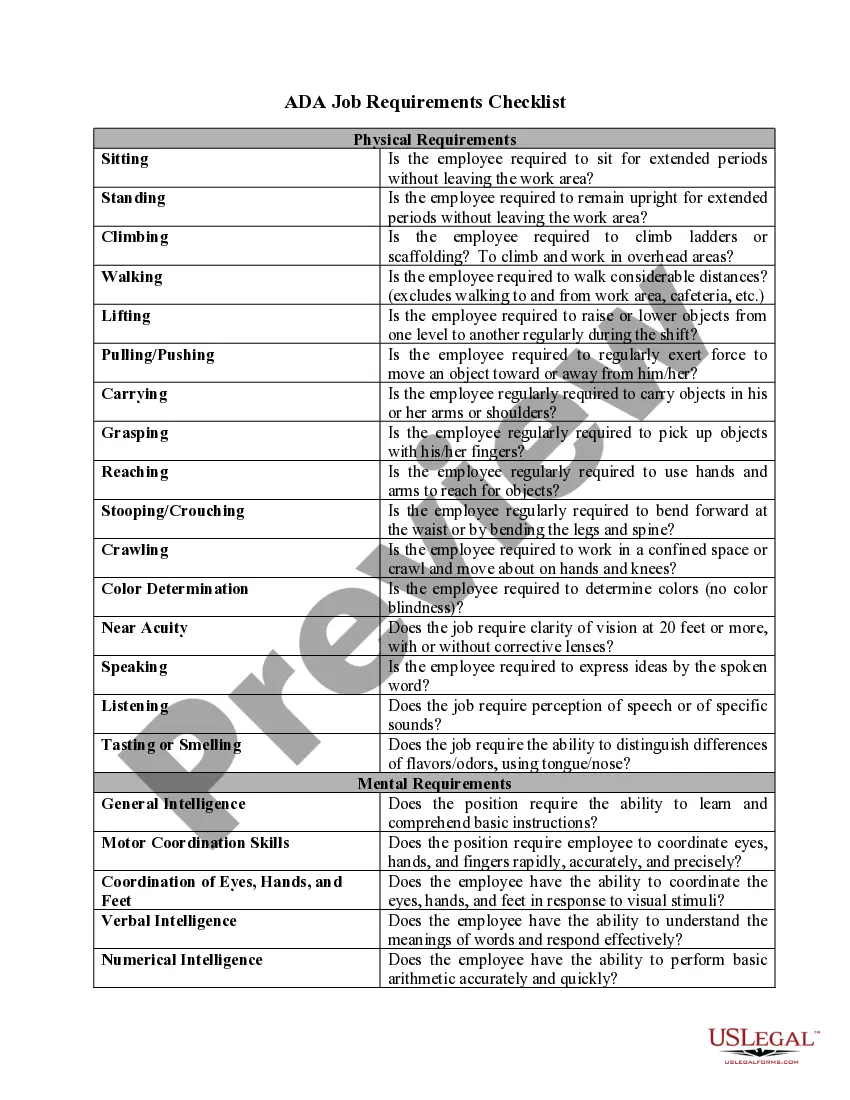
- Job description for the employee to provide context for the physician's evaluation.






When to use this document
This form should be utilized when an employer suspects that an employee's job performance issues may be related to a disability. It is particularly relevant in situations where the employer is considering reasonable accommodations and needs professional medical input to determine if a disability exists under the ADA.
Who can use this document
- Employers seeking to comply with ADA regulations when addressing employee performance concerns.
- Human resource professionals responsible for managing workplace accommodations.
- Physicians providing insights on employee disabilities as part of the accommodation process.
How to prepare this document
- Fill in the date and contact details for both the employer and physician.
- Provide the employee's name, position title, and a signed release for medical information.
- Clearly state the concerns regarding the employee's job performance and potential disability.
- Include the attached questionnaire for the physician with guiding questions.
- If necessary, provide the job description for context.
Is notarization required?
In most cases, this form does not require notarization. However, some jurisdictions or signing circumstances might. US Legal Forms offers online notarization powered by Notarize, accessible 24/7 for a quick, remote process.
Get your form ready online
Our built-in tools help you complete, sign, share, and store your documents in one place.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Make edits, fill in missing information, and update formatting in US Legal Forms—just like you would in MS Word.
Download a copy, print it, send it by email, or mail it via USPS—whatever works best for your next step.
Sign and collect signatures with our SignNow integration. Send to multiple recipients, set reminders, and more. Go Premium to unlock E-Sign.
If this form requires notarization, complete it online through a secure video call—no need to meet a notary in person or wait for an appointment.
We protect your documents and personal data by following strict security and privacy standards.
Common mistakes
- Not obtaining the employee's written consent before requesting medical information.
- Failing to provide clear context for the physician regarding the employee's job duties.
- Neglecting to follow up with the physician for timely responses.
Benefits of completing this form online
- Convenient access to legally vetted questionnaires anytime and anywhere.
- Edit and customize the form for specific employee situations quickly.
- Reliable support from licensed attorneys ensures compliance with ADA regulations.
Legal use & context
- This form is compliant with federal ADA standards and is used to assess employee disabilities.
- The information collected is to make determinations on reasonable accommodations required for the employee.
- All medical information collected is subject to confidentiality regulations under HIPAA.
Key takeaways
- The ADA Questionnaire for Physician aids employers in assessing potential disabilities in employees.
- Proper use of the form ensures compliance with ADA requirements and supports employee needs.
- Obtaining physician input is crucial for determining necessary workplace accommodations.
Looking for another form?
Form popularity
FAQ
What Leave is Required? ADA: Leave for employee may be required if it would constitute a reasonable accommodation that doesn't impose undue hardship on the employer. Leave typically must be for a defined period and is unpaid unless employer pays for other similar leaves.
This letter is in response to your request for an accommodation to perform the essential functions of your position.The health care provider's note that you provided to us on date stated that you have the following work restriction(s): list restrictions.
You can file an Americans with Disabilities Act (ADA) complaint alleging disability discrimination against a State or local government or a public accommodation (private business including, for example, a restaurant, doctor's office, retail store, hotel, etc.).
In order for you to prove that you were the victim of disability discrimination, you must first meet the criteria of a disability as defined by the ADA. To meet the definition, you must suffer from a mental or physical impairment that causes a substantial limitation of a major life activity.
The ADA requires an employer to provide reasonable accommodations to qualified individuals with disabilities who are employees or applicants for employment, unless to do so would cause an undue hardship on the operation of the employer's business.42 U.S.C.
Step 1 Create a policy. Step 2 Review your job descriptions. Step 3 Train your supervisors to recognize an accommodation request. Step 4 Arrange a personal meeting with the employee. Step 5 Consider whether you need information from the employee's physician. Step 6 Continue the dialogue.
The Americans with Disabilities Act (ADA) applies to employers with 15 or more workers. The Family and Medical Leave Act (FMLA) applies to all government employers (local, state and federal) and to private businesses with 50 or more workers within 75 miles (with some exceptions).
The Americans with Disability Act (ADA) protects people with disabilities from discrimination. Conditions that are minor and temporary (such as a cold or flu) don't count as disabilities under the ADA. However, a short-term illness or other impairment may qualify as a disability if it is severe.
A violation can occur when job postings discourage individuals with disabilities from applying, exclude them, or deny a qualified individual employment because of their disability. It is an ADA violation for any employer to demote, terminate, harass, or fail to provide reasonable accommodations to disabled employees.