Loading
Get Fmlacertificationservicemember.doc
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the FMLACertificationServiceMember.doc online
The FMLACertificationServiceMember.doc is an essential document for employees seeking leave to care for a service member with a serious injury or illness. This guide will provide you with clear instructions on how to accurately complete this form online.
Follow the steps to fill out the FMLACertificationServiceMember.doc online
- Click the ‘Get Form’ button to obtain the form and open it in the editor. This allows you to access the document and begin filling it out.
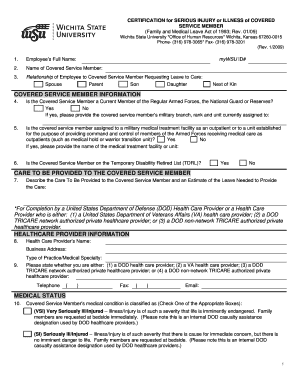
- Enter the employee’s full name and myWSU ID number in the designated fields at the top of the form.
- Provide the name of the covered service member who requires care.
- Indicate your relationship to the covered service member by selecting one of the options provided: spouse, parent, son, daughter, or next of kin.
- Answer the question regarding whether the covered service member is a current member of the Regular Armed Forces, the National Guard, or Reserves. If 'yes,' include their military branch, rank, and unit.
- Specify if the covered service member is assigned to a military medical treatment facility or a unit for outpatient care. If applicable, provide the name of the facility or unit.
- Indicate whether the covered service member is on the Temporary Disability Retired List (TDRL).
- Describe the care that will be provided to the covered service member and estimate the amount of leave needed.
- Fill in the healthcare provider’s information, including their name, business address, and type of practice or medical specialty.
- Classify the covered service member’s medical condition by checking the appropriate box based on the severity of their illness or injury.
- Answer whether the condition for which the covered service member is being treated was incurred in the line of duty on active duty.
- Provide the approximate date when the condition commenced.
- Estimate the probable duration of the condition and/or necessity for care.
- Indicate whether the covered service member is undergoing medical treatment, recuperation, or therapy, and describe it if applicable.
- State if the covered service member requires care for a continuous period, and estimate the beginning and ending dates if so.
- Indicate if they will need periodic follow-up treatment appointments, estimating the treatment schedule if applicable.
- Specify if there is a medical necessity for periodic care, and estimate the frequency and duration if it applies.
- Finally, the healthcare provider must sign and date the form.
- Once completed, save your changes and choose to download, print, or share the form as necessary.
Complete the FMLACertificationServiceMember.doc online to ensure you can provide the necessary care for your loved one.
FMLA itself does not allow employers to request your complete medical records. However, they can request specific information necessary for the FMLACertificationServiceMember.doc. This process helps protect your privacy while ensuring you provide adequate information needed to support your leave request.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.