Loading
Get Medicare Managed Care Reconsideration Background Data Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medicare managed care reconsideration background data form online
Filling out the Medicare managed care reconsideration background data form online can be straightforward when you know how to approach it. This guide will provide clear, step-by-step instructions to ensure you complete the form accurately and efficiently.
Follow the steps to successfully complete your form
- Click ‘Get Form’ button to obtain the form and open it in the editor.
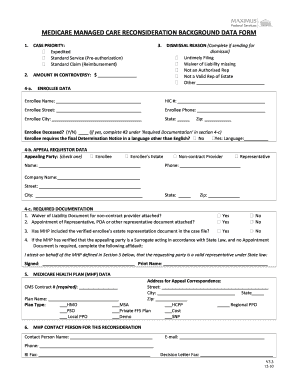
- Begin by selecting the case priority from the options: Expedited or Standard Service (Pre-authorization / Reimbursement). Ensure the correct option reflects your situation.
- Fill in the amount in controversy in the designated field, ensuring the dollar amount accurately represents the disputed claim.
- If applicable, complete the dismissal reason section by marking the reason for dismissal that applies to your case, such as untimely filing or waiver of liability missing.
- In the enrollee data section, provide the enrollee’s name, Health Insurance Claim Number (HIC), address, phone number, city, state, and zip code. Indicate whether the enrollee is deceased and, if applicable, if they require documentation in a language other than English.
- For the appealing party data, specify who is appealing by checking the appropriate box (enrollee, non-contract provider, or representative) and then fill in the required details, including contact information.
- Complete the required documentation section by confirming whether the necessary documents (such as waiver of liability) are attached and if the enrollee’s estate representation document is verified.
- In the Medicare health plan data section, provide the address for appeal correspondence and select the appropriate plan type corresponding to the enrollee’s Medicare health plan.
- Fill out the MHP contact person data with the relevant contact details. This includes the name, email, phone number, and fax information.
- Record all necessary dates related to the organization determination and reconsideration, ensuring accuracy in the MM/DD/YY format.
- Provide identification data for each provider involved, ensuring to complete a line for every provider and mark their relation to the MHP and any relevant dates.
- For denied services or claims, enter each item number, diagnosis, codes, and descriptions required to elaborate on the denial.
- Attach any supporting documentation as specified in the final section, including case narratives and MHP notice documents.
- Once all sections are filled out, review your entries for accuracy, then save your changes, download, print, or share the completed form as needed.
Start completing your Medicare managed care reconsideration background data form online today.
The MA organization must mail or otherwise transmit a written notice of the dismissal of the organization determination request to the parties. The notice must state all of the following: (1) The reason for the dismissal. (2) The right to request that the MA organization vacate the dismissal action.