Loading
Get Or Authorization To Release Medical Information 2021-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the OR Authorization To Release Medical Information online
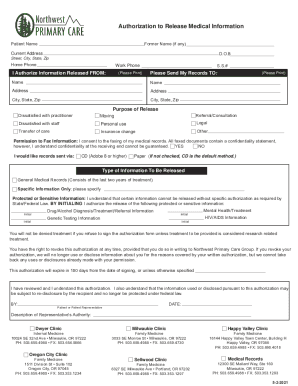
The OR Authorization To Release Medical Information form allows patients to securely share their medical records with designated parties. This guide will provide you with clear, step-by-step instructions to help you complete the form online, ensuring you can manage your medical information efficiently.
Follow the steps to successfully complete the form.
- Press the ‘Get Form’ button to access the form and open it for editing.
- Enter your personal information in the designated fields. This includes your patient name, former name if applicable, current address, date of birth, and contact numbers (home and work). Ensure all entries are legible.
- Indicate the source of the medical information being released by filling out the 'I Authorize Information Released FROM:' section, including the name and social security number if required.
- Specify where you would like the records sent by completing the 'Please Send My Records TO:' section, including the name, address, city, state, and zip code.
- Select the purpose for the release of information from the provided options, such as personal use, transfer of care, or referral/consultation.
- If applicable, indicate your permission for the information to be faxed by selecting 'YES' or 'NO'. Be aware of the confidentiality considerations regarding faxed documents.
- Choose how you prefer to receive your records—via CD or paper—and check the respective option. If not specified, a CD will be the default method.
- Identify the type of information you wish to release by selecting either general medical records or specifying particular information. If requesting sensitive information, initial the corresponding sections to authorize the release.
- Review the authorization conditions carefully. Understand that you can revoke this authorization in writing and that it will expire in 180 days unless otherwise specified.
- Finally, sign and date the form at the bottom section. If you are completing this on behalf of someone else, describe your authority to do so.
- Once you have completed all sections and confirmed accuracy, you can save your changes, download the form, print it, or share it as needed.
Take control of your medical information by completing the OR Authorization To Release Medical Information form online today.
Should I sign this “HIPAA Authorization” for release of my medical records? No, you should not sign the HIPAA authorization for the release of your medical records. Often, the insurance company will act as though they cannot begin to decide how much money to offer you until they have all of your medical records.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.