Loading
Get Cshcn Service Program Wheelchair Seating Evaluation Form Pdf
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Cshcn Service Program Wheelchair Seating Evaluation Form Pdf online
Filling out the Cshcn Service Program Wheelchair Seating Evaluation Form Pdf online is an essential step for individuals seeking wheelchair seating evaluations. This guide provides a user-friendly overview of the form and detailed instructions to ensure a thorough completion.
Follow the steps to successfully complete the evaluation form online.
- Press the ‘Get Form’ button to obtain the Cshcn Service Program Wheelchair Seating Evaluation Form and open it in your preferred online editor.
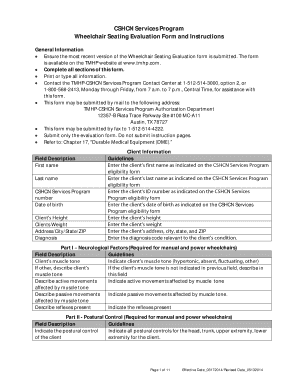
- Begin by filling out the client information section. Provide the first name, last name, CSHCN Services Program number, date of birth, address, and relevant diagnosis. Ensure accuracy and completeness of all details.
- Proceed to Part I, Neurological Factors. Describe the active and passive movements affected by muscle tone and any reflexes present. This information is crucial for understanding the client’s needs.
- In Part II, Postural Control, indicate the level of head, trunk, upper extremity, and lower extremity control. Use the options given to provide a clear profile of the client’s postural capabilities.
- Move to Part III, Medical/Surgical History and Plans. Answer questions regarding skin integrity, orthopedic conditions, and any anticipated surgeries. Be detailed in your explanations to provide context for the evaluation.
- Complete Part IV, Functional Assessment, by indicating the client’s ambulatory status, dependency on a wheelchair, and feeding capabilities. This helps establish the functional needs of the client.
- In Part V, Environmental Assessment, describe the accessibility of the client’s home and school environment. This information will assist in determining the suitability of recommended equipment.
- Move to Part VI, Requested Equipment. Indicate the wheelchair type, serial number, purchase date, and medical necessity for the requested equipment. Provide a clear justification for any modifications needed.
- If applicable, complete Part VII for Power Wheelchairs. Describe the medical necessity for a power wheelchair and how it will be operated. Ensure that all questions are answered comprehensively.
- Lastly, ensure that the therapist signs the form, indicating their qualification to assess and recommend the equipment needed. Save your changes and download, print, or share the completed form as necessary.
Ready to complete your document? Fill out the Cshcn Service Program Wheelchair Seating Evaluation Form Pdf online now.
Related links form
Create Their Own Forms As Long As - Alaska Child Support ... - Csed State Ak
True North Project Reclamation Plan - Alaska Department Of Natural ...
025 Employee Discipline Effective: November 1, 2009 Page 2 Of 20 Oral Instructions And Written
U.S. Fish And Wildlife Service Form 3-200-10b - Alaska Department ...
Wheelchair Evaluation Seat width, depth, and height. Patient hip, trunk, and shoulder widths. Patient shoulder and axillae heights. WC Leg length, arm height, back height. WC width, height, and size. Knee-to-seat depth. Knee-to-heel length. Seat-to-back support angle.