Loading
Get Medicare Part D Coverage Determination Request Form. Medicare Part D Coverage Determination Request
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medicare Part D Coverage Determination Request Form online
Filling out the Medicare Part D Coverage Determination Request Form accurately is essential for obtaining the necessary medication coverage. This guide will walk you through each section of the form to ensure a smooth and efficient process.
Follow the steps to complete your request form effectively.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
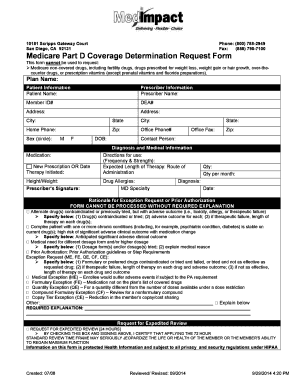
- Begin by entering the plan name in the designated field to identify which Medicare plan you are associated with.
- Fill out the patient information section. Include the patient’s name, member ID number, date of birth, home phone number, and address.
- In the prescriber information section, input the prescriber's name, address, and contact details including DEA number, office phone, and fax number.
- Next, provide details about the medication requested. Indicate whether this is a new prescription or for an ongoing therapy, along with the therapy initiation date.
- Include the patient's height and weight, medication direction for use (frequency and strength), and expected length of therapy.
- Detail any known drug allergies and the requested quantity for the medication, specifying how many units are needed per month.
- In the diagnosis section, provide a clear statement of the medical condition relevant to the medication request.
- Complete the rationale for the exception request field, explaining why an exemption or prior authorization is necessary and detailing any previous medications tried, including adverse outcomes.
- If applicable, check the box for expedited review if waiting would jeopardize the patient’s health and sign where indicated.
- Finally, review all entered information for accuracy. Once confirmed, save your changes, and consider downloading, printing, or sharing the completed form as needed.
Complete your documents online for prompt processing.
The Secretary of the Department of Health and Human Services determines whether a particular item or service is covered nationally by Medicare, which essentially grants, limits or excludes national coverage to all Medicare beneficiaries.