Loading
Get Umr Ez Claim Form Medical/vision
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the UMR EZ Claim Form Medical/Vision online
The UMR EZ Claim Form Medical/Vision is designed to help users easily submit medical and vision claims. This guide provides clear step-by-step instructions to ensure you successfully complete the form online, facilitating a smooth claims process.
Follow the steps to complete your claim form online.
- Press the ‘Get Form’ button to access the UMR EZ Claim Form Medical/Vision. This will allow you to open the form in an online editor.
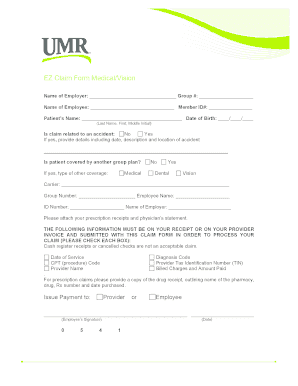
- Fill in the Employer's name and the Group number in the designated fields.
- Enter your full name as the employee along with your Member ID number.
- Provide the patient's name and date of birth, clearly separating the last name, first name, and middle initial.
- Indicate whether the claim is related to an accident by selecting 'Yes' or 'No'. If 'Yes', describe the details of the accident, including the date, description, and location.
- Next, state if the patient has coverage under another group plan by selecting 'Yes' or 'No'. If 'Yes', fill out the type of coverage and complete the section for carrier information.
- Ensure to attach the required prescription receipts and a physician’s statement, as specified. Verify that the necessary information is included on your receipts for processing.
- Complete the 'Issue Payment to' section, choosing either the provider or employee.
- Sign the form with your name and date.
- Once you have filled out the form completely, save any changes, and then download or print the form as necessary. You can also share it as needed.
Complete your UMR EZ Claim Form Medical/Vision online today for a streamlined claims process.
Related links form
You can reach the UnitedHealthcare vision department at 1-800-638-3120. This number is available for questions related to your vision insurance, including inquiry regarding claims and coverage. It's always a good idea to have your policy information handy when you call to streamline the process.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.