Loading
Get Patient Assistance Program Application Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Patient Assistance Program Application Form online
Completing the Patient Assistance Program Application Form online can be a straightforward process if you follow the appropriate steps. This guide provides comprehensive instructions to assist both patients and physicians in filling out the required information accurately and efficiently.
Follow the steps to complete your application form successfully.
- Click ‘Get Form’ button to obtain the form and open it in the document editor.
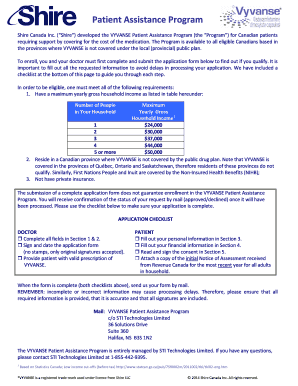
- Sections 1 and 2 should be completed by the physician. This includes providing patient information such as first name, last name, date of birth, treatment details, and dosage requested for . Ensure that all fields are filled out clearly and legibly.
- In Section 2, the physician must include their own details including name, address, contact information, and license number. The physician must provide an original signature to consent to the information collection.
- Patients or their legal guardians should proceed to Section 3 after the physician's information is complete. Fill out the personal information about the patient, including first name, last name, date of birth, address, and contact details.
- In Section 4, provide answers to questions regarding private insurance status, First Nations or Inuit identity, the number of people in the household, and the yearly gross household income. Attach a copy of the initial Notice of Assessment from Revenue Canada for the most recent year for each adult in the household.
- Complete Section 5 by signing the consent form. This section allows for the collection, use, and disclosure of personal and medical information for the Patient Assistance Program.
- After all sections are filled out completely, review the application for accuracy and completeness. Incomplete or incorrect information may result in processing delays.
- Finally, send the completed form by mail to the designated address provided at the bottom of the application form.
Take the first step towards assistance by completing the Patient Assistance Program Application Form online today.
That's why we offer myAbbVie Assist, our patient assistance program that provides free AbbVie medicines to qualifying patients....Income criteria for myAbbVie Assist. Household sizeAnnual income2$104,520 or less3$131,760 or less4$159,000 or less1 more row