Loading
Get Ha-0889-1115 Active Local Gov App Layout 1
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Ha-0889-1115 Active Local Gov App Layout 1 online
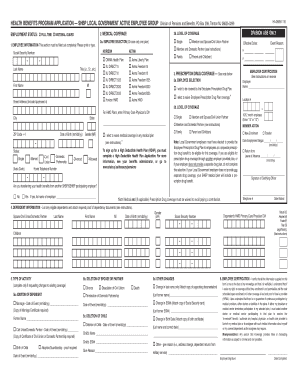
The Ha-0889-1115 Active Local Gov App is an essential form for local government employees seeking health benefits. This guide provides comprehensive instructions on how to accurately complete the application online, ensuring all necessary information is submitted for processing.
Follow the steps to complete the application process effectively.
- Click ‘Get Form’ button to obtain the form and open it in your online editor.
- In section 1, provide your full employee information. This includes entering your last name, first name, middle initial, Social Security number, and employment status. Make sure all fields are accurately filled out.
- In section 2, select your preferred medical coverage. Choose one from the provided plans and indicate the desired level of coverage (single, member and spouse, etc.). Ensure that you check only one box in each subsection.
- Proceed to section 3 regarding prescription drug coverage. Indicate whether you wish to be covered by the Employee Prescription Drug Plan or if you choose to waive this coverage.
- In section 4, list all eligible dependents you wish to cover. Provide the required information for each dependent, including their name, date of birth, gender, and Social Security number. Ensure you attach any necessary proof of dependency.
- If you are making any changes in section 5, check the appropriate boxes to indicate the type of activity (adding or deleting dependents). Fill in the required dates and details as needed.
- In section 6, you must certify your information. Read the employee certification statement thoroughly, then sign and date the application.
- Once all sections are completed, ensure everything is accurate. You can then save your changes, download the form, print it, or share it as necessary.
Complete your health benefits application online today to ensure timely processing!
About the Program The Empire Plan is the primary health insurance plan for NYSHIP, covering 1.1 million members. Civil Service contracts with UnitedHealthcare Insurance Company of New York (United) to administer the Empire Plan's medical/surgical benefits.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.