Loading
Get When Completed Please Mail This Form And Attachments To P
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the When Completed Please Mail This Form And Attachments To P online
Filling out the When Completed Please Mail This Form And Attachments To P can seem daunting, but this guide will help you navigate through the process with ease. By following these straightforward steps, you can ensure that your submission is complete and accurate.
Follow the steps to effectively complete the form online.
- Click ‘Get Form’ button to access the necessary form and open it in the editor.
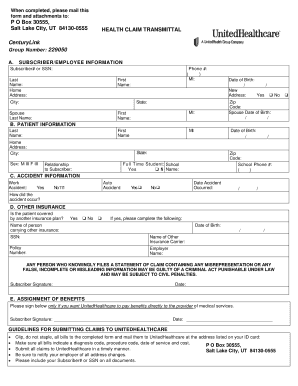
- Begin with Section A: Subscriber/Employee Information. Enter your subscriber number or Social Security Number (SSN), last name, first name, middle initial (if applicable), home address, city, state, and zip code. Don't forget to include your phone number.
- If applicable, provide your spouse's last name, first name, middle initial, and date of birth. Indicate if there is a new address by selecting 'Yes' or 'No'.
- Move on to Section B: Patient Information. Fill in the patient's last name, home address, city, state, zip code, and school phone number. Specify the patient's sex and date of birth. If the patient is a full-time student, select 'Yes' or 'No' and include the name of their school.
- In Section C: Accident Information, indicate whether the accident was a work-related or auto accident. Provide the date of the accident and a brief explanation of how it occurred.
- Proceed to Section D: Other Insurance. Indicate if the patient is covered by another insurance plan, selecting 'Yes' or 'No.' If applicable, provide details including the name of the person carrying the other insurance, their date of birth, Social Security Number, name of the other insurance carrier, policy number, and employer name.
- In the signature area, ensure you sign and date the form in the Subscriber Signature section, confirming that the information is accurate and true to your knowledge.
- If you wish for benefits to be paid directly to the provider of medical services, sign in the Assignment of Benefits section; otherwise, you can leave it blank.
- Finally, before submitting, clip all bills to the completed form (do not staple) and ensure that all required information is included. Save or download the completed form, then print it for mailing.
Complete your documents online today for a more efficient submission process!
Click the Data tab. Under Binding, click Specify default file, and then click Browse. In the Attach File dialog box, select the file that you want to appear inside the file attachment box on the form template, and then click Insert.