Loading
Get Guide To Resolving Health Insurance Problems ... - State Of ...
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the Guide To Resolving Health Insurance Problems online
Filling out the Guide To Resolving Health Insurance Problems is essential for effectively addressing health insurance issues. This comprehensive guide will walk you through each step of the process to ensure that users can navigate the form effortlessly and accurately.
Follow the steps to complete your health insurance problems guide online.
- Press the ‘Get Form’ button to obtain the form and open it in the designated editor.
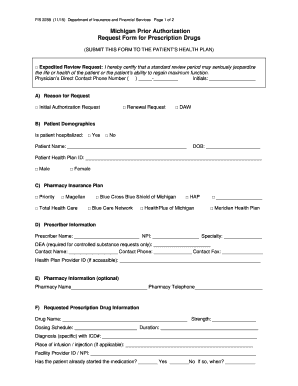
- Begin by selecting the reason for your request. Choose from options such as renewal request, initial authorization request, or other (DAW). This information is essential for processing your request accurately.
- Fill out the patient demographics section. Include the patient’s name, date of birth, health plan ID, and gender. This helps in identifying the patient and linking them to their health insurance plan.
- Complete the pharmacy insurance plan section by selecting the appropriate insurance provider from the listed options. This is important for determining coverage.
- Provide the prescriber information. Enter the prescriber’s name, NPI number, specialty, and contact information. If the request is for a controlled substance, you will need to fill in the DEA number.
- If applicable, include the pharmacy's information such as name and telephone number to ensure prompt communication regarding the prescription.
- Specify the requested prescription drug information. Fill in the drug name, strength, dosing schedule, duration of treatment, diagnosis with ICD number, and any relevant details about where the drug will be administered.
- In the rationale for prior authorization section, provide necessary background information such as the patient’s medical history, previous medications, and any other details that support your request.
- List any failed or contraindicated therapies by providing the drug name, strength, dosing schedule, duration, and details about any adverse events.
- If necessary, fill out the optional section for other pertinent information. This may include diagnostic labs or measures of treatment response that could assist in the review.
- Finally, certify the accuracy of the information provided by signing and dating the form. Ensure all sections are completed to avoid delays.
- After completing the form, review your entries for accuracy. Save any changes, and then you can download, print, or share the form as needed.
Complete your documents online today to effectively resolve your health insurance problems.
Related links form
How to write this complaint letter: Give all the relevant facts concerning the claim. Refer to any documents that will help substantiate your position. Include a specific request for action you feel will correct the situation. ... Close the letter with an expression of hope or confidence.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.