Loading
Get Blue Cross Blue Shield Of Arizona Provider Change Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Blue Cross Blue Shield Of Arizona Provider Change Form online
Filling out the Blue Cross Blue Shield Of Arizona Provider Change Form is a straightforward process that ensures your provider information is accurate and up-to-date. This guide provides clear, step-by-step instructions to help you complete the form efficiently and effectively.
Follow the steps to successfully fill out your Provider Change Form
- Click ‘Get Form’ button to obtain the form and open it in the editor.
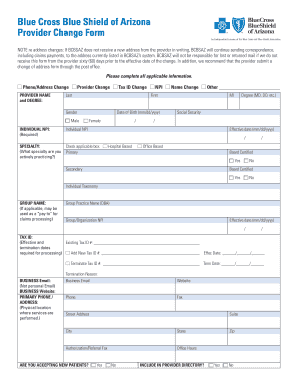
- Begin by entering your provider information. Fill in your full name, including your last name, first name, and middle initial. Specify your degree, such as MD or DO, and provide your individual NPI number along with your date of birth.
- Select the applicable change type, such as phone/address change, provider change, tax ID change, last name change, or any other reason. Ensure to check the box next to the relevant option.
- Indicate your specialty and whether you are board certified. This includes checking the appropriate boxes to reflect your primary or secondary practice status.
- If applicable, provide the group name and group organization NPI. Include the effective date of any changes being made.
- Complete the section on tax identification by entering your existing and any new tax ID numbers, along with effective and termination dates when necessary.
- Fill in your primary phone and address details, including the street address, suite, city, state, and zip code where services are performed.
- Indicate whether you are accepting new patients and if you wish to be included in the provider directory by checking the appropriate boxes.
- Complete the billing and mailing address sections similarly, providing the necessary details where payments and correspondence will be sent.
- If you have additional offices, include those details on an attached sheet, as needed.
- Provide information about medical records if they are different from your primary location.
- In the section for hospital or free-standing surgery facility privileges, indicate the status of your privileges.
- Enter your authorized electronic signature in the designated field, verifying your authority to submit the form on behalf of the provider.
- Finalize by saving changes, then submit the form via email or fax as indicated at the bottom of the document.
Ensure your provider information is current by completing your documents online today.
Related links form
Call your closest office: (602) 864-4884, or toll-free (800) 232-2345, ext. 4884 Do you speak Spanish? Our service department does, too.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.