Get Insurance Verification Form Date Name Of Provider In - Goldstarmedical
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the INSURANCE VERIFICATION FORM DATE NAME OF PROVIDER IN - Goldstarmedical online
Filling out the insurance verification form accurately is essential for ensuring that your coverage is confirmed and the necessary services are authorized. This guide will walk you through each section of the form to help streamline the process.
Follow the steps to complete the insurance verification form effectively.
- Click the ‘Get Form’ button to obtain the form and open it in your preferred document editor.
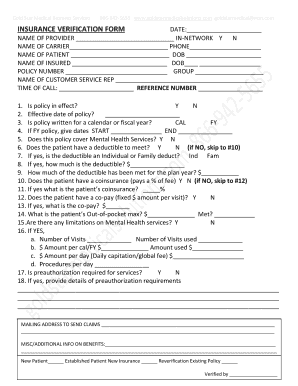
- In the 'DATE' section at the top of the form, enter the current date to indicate when the verification is being completed.
- Fill in the 'NAME OF CARRIER' section with the name of the insurance company. Then, include the 'PHONE' number associated with the insurance carrier for any follow-up verification.
- In the 'NAME OF INSURED' section, write the name of the person who holds the insurance policy, along with their date of birth.
- Provide the name of the customer service representative you spoke with for this verification in the 'NAME OF CUSTOMER SERVICE REP' section.
- Answer the questions regarding the policy status, effective date, and whether the policy is written for a calendar or fiscal year, marking with 'Y' or 'N' as appropriate.
- Complete all sections regarding mental health services coverage, including any limitations, preauthorization requirements, and additional information necessary for claim processing.
- After filling in all sections, you can save any changes made, download the form for personal records, print it for submission, or share it electronically as needed.
Start filling out your insurance verification form online today to ensure quick and accurate service!
To fill out insurance claim form part A, begin by entering your personal information, such as name, address, and policy number. Make sure to provide accurate details that match your insurance documents to avoid any delays. You can refer to the guidelines included with the form or use the INSURANCE VERIFICATION FORM DATE NAME OF PROVIDER IN - Goldstarmedical as a reference to ensure all required fields are completed correctly.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.