Get Neuron Reimbursement Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Neuron Reimbursement Form online
Filling out the Neuron Reimbursement Form online is a straightforward process designed to streamline your reimbursement claims. This guide provides a step-by-step approach to ensure that users can complete the form efficiently and accurately.
Follow the steps to successfully complete the Neuron Reimbursement Form.
- Click ‘Get Form’ button to obtain the document and open it for editing.
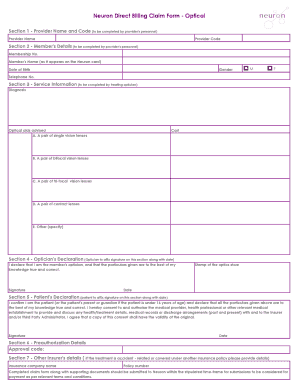
- In Section 1, enter the provider's name and code, which should be completed by the provider's personnel.
- Move to Section 2 to input the member's details. This includes the membership number, the member's name as it appears on the Neuron card, date of birth, gender (select M or F), and telephone number. Ensure accuracy in this section to avoid processing delays.
- Proceed to Section 3, where the treating optician will complete the service information. This includes the diagnosis and the recommended optical aids. Specify the cost for each type of lenses requested: single vision lenses, bifocal lenses, tri-focal lenses, contact lenses, or any other specified optical aids.
- In Section 4, the optician must provide their declaration by signing and dating the document. The stamp of the optics store should also be affixed here.
- Next, Section 5 is to be completed by the patient. The patient (or the patient's parent/guardian if under 16) should sign and date this section, confirming the accuracy of the details and providing consent for information sharing with relevant parties.
- Section 6 requires the preauthorization details where you will input the approval code.
- Finally, if the treatment is related to an accident or covered under another insurance policy, fill in Section 7 with the insurance company name and policy number.
- After filling in all sections, review the form for completeness and accuracy. Users can then save changes, download, print, or share the form as needed.
Complete your Neuron Reimbursement Form online today for a smooth processing experience.
To fill out a motor claim form, begin by gathering all necessary documentation related to the incident, including your policy number and details about the accident. Clearly write out the date, time, and location of the event, and provide a description of what occurred. Make sure to include any witness information and relevant damages. If you are using the Neuron Reimbursement Form for reimbursements related to this incident, ensure you attach all related receipts.