Get Guthrie Authorization To Use Or Disclose Health Information
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Guthrie Authorization to Use or Disclose Health Information online
Filling out the Guthrie Authorization to Use or Disclose Health Information form online is a critical step in managing your healthcare information. This guide will provide you with clear instructions to ensure that you complete the form accurately and efficiently.
Follow the steps to complete the authorization form effectively.
- Click ‘Get Form’ button to obtain the form and open it in the digital editor.
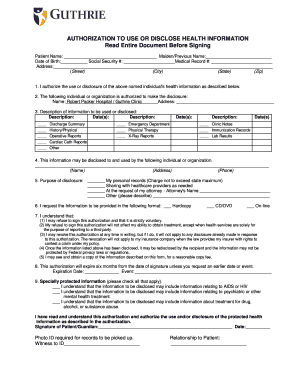
- Begin by filling in your personal details. Provide your full name, any previous name, date of birth, social security number, medical record number, and your current address including street, city, state, and zip code.
- In the section labeled 'I authorize the use or disclosure of the above named individual's health information as described below,' ensure you clearly state the intended purpose of the authorization.
- Identify the individual or organization authorized to make the disclosure. For this form, it is Robert Packer Hospital / Guthrie Clinic. Fill in the address for the organization.
- Describe the specific information to be disclosed by checking the appropriate boxes such as 'Discharge Summary,' 'Emergency Department,' 'Clinic Notes,' and provide any additional descriptions and dates as necessary.
- Indicate the recipient of the information by providing their name, address, and phone number in the designated fields.
- Specify the purpose of the disclosure by checking one or more of the options provided: personal records, sharing with healthcare providers, attorney request, or other. If other, include a brief description.
- Request the format in which you would like to receive the information; options include hardcopy, CD/DVD, or online.
- Carefully read the consent statements and confirm your understanding by acknowledging that signing the authorization is voluntary and can be revoked at any time. Take note that once disclosed, the information may not be protected by privacy laws.
- Include the expiration date for the authorization, which can be up to six months from the date of signature, or indicate a specific event for its expiration.
- If applicable, check any boxes related to specially protected information such as AIDS, mental health treatment, or substance abuse, and acknowledge understanding of these disclosures.
- Finally, sign the form as the patient or guardian, add the date, and ensure any necessary photo ID is ready for record pickup.
- After completing all sections, you can save your changes, download the completed form, print it, or share it as needed.
Start filling out the Guthrie Authorization to Use or Disclose Health Information online today to take control of your healthcare management.
An authorization to release information must include the patient’s full name, the specific records to be released, the purpose of the request, and the recipient's name. You also need to include the expiration date of the authorization and a signature to indicate consent. This ensures that all parties are clear on what information is being shared and why, which is essential for protecting patient privacy. The Guthrie Authorization to Use or Disclose Health Information can help you format and complete this accurately.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.