Loading
Get Instructions For Physician's Report.qxd - Colorado Department Of Labor
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Instructions For Physician's Report.qxd - Colorado Department Of Labor online
Filling out the Instructions For Physician's Report provided by the Colorado Department of Labor is essential for reporting workplace injuries effectively. This guide will walk you through each section of the form, ensuring you provide the necessary information accurately and efficiently.
Follow the steps to complete the physician's report accurately.
- Click the ‘Get Form’ button to access the form digitally and open it in an online editor.
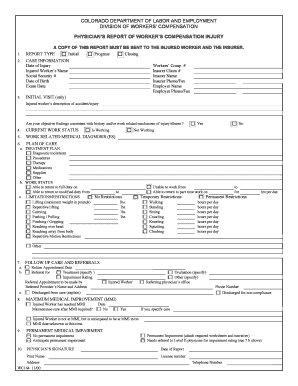
- Begin with the Report Type section. Indicate whether this report is 'Initial,' 'Progress,' or 'Closing' by clicking the appropriate checkbox.
- In the Case Information section, fill in the required fields such as Date of Injury, Injured Worker’s Name, Social Security Number, Date of Birth, Exam Date, Workers’ Comp Number, Insurer Claim Number, Insurer Name, and both Employer details.
- For the Initial Visit section, provide a description of the accident or injury using the injured worker's own words. Additionally, select whether the objective findings are consistent with the history provided.
- Next, select the Current Work Status of the injured worker, indicating whether they are working or not.
- In the Work Related Medical Diagnosis section, list the medical diagnoses related to the workplace injury.
- For the Plan of Care, detail the treatment plan, including diagnostic tools, procedures, therapy options, medications, and any necessary supplies.
- Indicate the Work Status, specifying if the injured worker can return to full duty or needs modifications. Provide any limitations or restrictions on activities.
- Complete the Follow Up Care and Referrals section, including return appointment dates and any referrals made to other healthcare providers.
- In the Maximum Medical Improvement (MMI) section, check the appropriate box and specify if the injured worker has reached MMI or if further treatment is required.
- Address the Permanent Medical Impairment question by checking the relevant box and, if applicable, noting the need for an impairment rating from a qualified physician.
- Finally, sign the report by providing your name, license number, and contact information. Ensure you date the report appropriately.
- Once you have filled out all applicable fields, you can save changes, print, download, or share the completed form as necessary.
Complete your documents online today to ensure efficient and compliant reporting.
No Admission of Liability. The settlement evidenced by this Agreement is not an admission of liability or wrongdoing or noncompliance with any federal, state, city or local rule, ordinance, statute, contract, public policy or any unlawful conduct or breach of any duty whatsoever by any party.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.