Loading
Get Massachusetts Standard Form For Medication Prior ... - Mass.gov
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Massachusetts Standard Form For Medication Prior Authorization online
Navigating the Massachusetts Standard Form For Medication Prior Authorization can feel complex. This guide will walk you through each section and field of the form, providing clear instructions to help you complete it successfully.
Follow the steps to fill out the form accurately.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
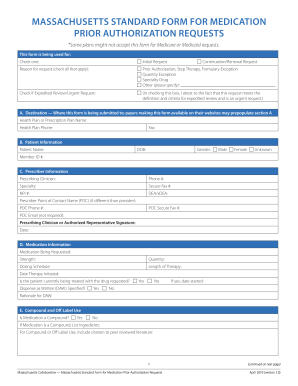
- Select the type of request by checking either 'Initial Request' or 'Continuation/Renewal Request'. Indicate the reason for the request by checking all applicable options, including prior authorization, step therapy, quantity exception, specialty drug, or specify any other reason.
- If applicable, check the box for expedited review/urgent request and ensure you attest that the criteria for expedited review have been met.
- Complete section A with the health plan or prescription plan name and their contact information, including phone and fax numbers.
- Fill in patient information in section B, including their name, date of birth, gender, and member ID number.
- In section C, provide prescriber information, including the prescribing clinician's name, phone, specialty, and secure fax number. Include the prescriber’s NPI and DEA/xDEA numbers, as well as point of contact details if they differ from the provider.
- In section D, provide specific medication details such as the requested medication, strength, quantity, dosing schedule, and length of therapy. Indicate if the patient is currently being treated with this medication.
- In section E, indicate if the medication is a compound and list the ingredients if applicable. For off-label use, include citations to peer-reviewed literature.
- In section F, provide patient clinical information, including primary diagnosis related to the medication request, relevant comorbidities, drug allergies, height, and weight. Fill in any pertinent concurrent medications and previous therapies tried.
- Include additional information regarding professional administered medications. Specify start and end dates, servicing provider details, and any billing provider information.
- Review all entered information for accuracy before you save your changes, download, print, or share the completed form.
Prepare your documents online with these straightforward steps today.
Prior authorization helps Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) suppliers ensure that applicable Medicare coverage, payment, and coding rules are met before DMEPOS items are delivered.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.