Loading
Get Family Physician Insurance Program Aafp Member ...
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the FAMILY PHYSICIAN INSURANCE PROGRAM AAFP MEMBER form online
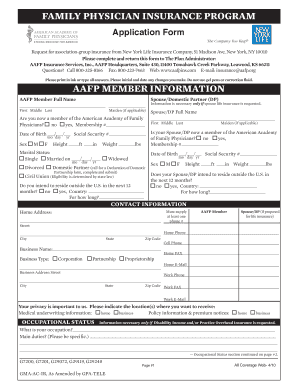
Filling out the FAMILY PHYSICIAN INSURANCE PROGRAM application form is an essential step for AAFP members seeking insurance coverage. This guide will provide you with clear, step-by-step instructions to complete the form efficiently and accurately online.
Follow the steps to successfully complete your insurance application.
- Click the ‘Get Form’ button to obtain the form and open it in the editor.
- Fill out the AAFP Member Information section. Start with your full name, followed by your spouse/domestic partner's name if applicable. Ensure you provide your membership number if you are a member of the American Academy of Family Physicians.
- Complete the Date of Birth, Social Security number, Sex, Height, Weight, and Marital Status fields. Only complete the spouse/domestic partner information if you are applying for their life insurance.
- Provide your contact information, including your home address, phone numbers, and email addresses. Ensure to mark the preferred location for receiving medical underwriting and policy information.
- In the Occupational Status section, specify your occupation and main duties. Confirm whether you are working full-time as per the guidelines provided.
- Indicate your preferred payment options for insurance, including billing method and frequency. Review the options carefully to select what works best for you.
- In the Life Insurance Requested section, indicate the coverage amounts you are applying for, ensuring you understand the limits and conditions stated.
- Fill out the Beneficiary Designation section, specifying who will receive the insurance proceeds. Provide name, address, relationship, and social security numbers as required.
- If applicable, fill out the Disability Income Insurance Requested and Practice Overhead Insurance Requested sections, providing details as prompted.
- Review all information for accuracy. Sign and date the application. If the spouse/domestic partner is included in the coverage, their signature is also required.
- Once completed, you can save changes, download, print, or share the application form.
Complete your FAMILY PHYSICIAN INSURANCE PROGRAM application online today to ensure you and your loved ones are protected.
All of the AAFP Foundation's efforts are made possible through the donations of family physicians, corporations and others who provide voluntary financial support for the AAFP Foundation. Who We Are - The AAFP Foundation aafpfoundation.org https://.aafpfoundation.org › who-we-are aafpfoundation.org https://.aafpfoundation.org › who-we-are
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.