Loading
Get Worker's Claim For Compensation
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WORKER'S CLAIM FOR COMPENSATION online
Filling out the worker's claim for compensation is an essential step for employees who have sustained an injury or illness related to their work. This guide provides clear and supportive instructions to help users complete the form accurately and effectively.
Follow the steps to fill out the form correctly and efficiently.
- Click 'Get Form' button to obtain the form and open it in the desired format.
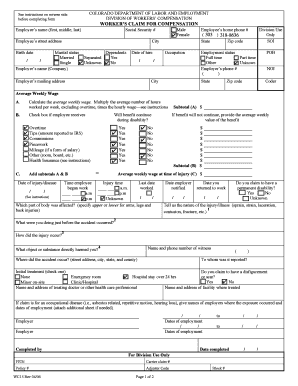
- Enter your name in the first, middle, and last name fields. Ensure the spelling is accurate.
- Provide your Social Security number in the corresponding field, ensuring it's entered correctly.
- Fill in your street address, city, state, and zip code. Review for accuracy.
- Select your gender by checking the appropriate box: 'Male' or 'Female'.
- Enter your birth date in the specified format (MM/DD/YYYY).
- Indicate your marital status by checking one of the options provided.
- List any dependents you may have by checking 'Yes' or 'No'.
- Enter your employer’s name and the date you were hired, ensuring accurate information.
- Provide your occupation and employer’s mailing address, including city and zip code.
- Fill in your home phone number accurately, ensuring it is current.
- Indicate your employment status by selecting 'Full time,' 'Part time,' or 'Other.'
- Calculate and enter your average weekly wage by following the instructions provided in the form.
- Document the details of your injury including the date, time, and description of the injury.
- Describe how the injury occurred and what you were doing just before it happened.
- Provide contact information for any witnesses to the incident.
- Indicate the nature of any treatment received and the name and address of the treating doctor.
- Complete the rest of the form as instructed, reviewing each section to ensure all fields are filled.
- Once all sections are completed, review the form for any errors or omissions.
- Save changes, download, print, or share the form as needed according to your preferences.
Complete your worker's claim for compensation online today.
Workers' compensation is insurance, paid for by your employer, that provides cash benefits and medical care if you become disabled because of an injury or illness related to performing your job. All State employees are covered by the Workers' Compensation Law.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.