Loading
Get Pain Programs Review Form - Healthpartners
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Pain Programs Review Form - HealthPartners online
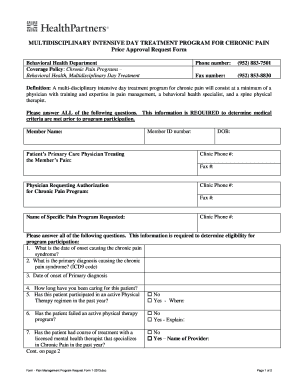
The Pain Programs Review Form - HealthPartners is an essential document for those seeking approval for participation in multidisciplinary day treatment programs for chronic pain. This guide provides a step-by-step approach to filling out the form accurately and effectively.
Follow the steps to complete the form online with ease.
- Click ‘Get Form’ button to acquire the Pain Programs Review Form - HealthPartners and open it in an appropriate editor.
- Begin by entering the member name and member ID number in the specified fields. Ensure accuracy as this information is crucial for identification.
- Fill in the patient's primary care physician's name and contact information, including clinic phone number and fax number.
- Enter the name of the physician requesting authorization for the chronic pain program along with their clinic phone number and fax number.
- In the section pertaining to the specific pain program requested, clearly state the name of the program.
- Respond to the questions regarding the date of onset of the chronic pain syndrome, primary diagnosis, and dates associated with these conditions.
- Detail the duration of care provided for the patient and confirm whether the patient has participated in an active physical therapy regimen in the past year.
- Indicate if the patient has failed an active physical therapy program and provide explanations where necessary.
- Answer the questions regarding any treatment the patient has received from a licensed mental health therapist specializing in chronic pain. Include the therapist's name if applicable.
- List current medications that the patient is taking, ensuring to provide complete details for each.
- Confirm whether the patient has been evaluated by a physician specializing in chronic pain in the past year.
- Enumerate the medical interventions the patient has undergone, providing the name of the provider if available.
- Describe the expected outcomes from the patient's participation in the program.
- Confirm if the requesting physician will collaborate with the pain program post-treatment and provide details if another physician will follow the patient.
- Finally, print the name, sign, and date the form. Ensure that the completed form is faxed back to Behavioral Health at the provided number.
Complete your Pain Programs Review Form - HealthPartners online today to ensure timely processing of your request.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.