Loading
Get Hospital Confinement Policy Application & Change Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the HOSPITAL CONFINEMENT POLICY APPLICATION & CHANGE FORM online
This guide provides a comprehensive approach to completing the Hospital Confinement Policy Application & Change Form online. Users can follow these detailed instructions to ensure their application is submitted accurately and efficiently.
Follow the steps to successfully complete your application online.
- Press the ‘Get Form’ button to access the Hospital Confinement Policy Application & Change Form. This will open the form in your designated online form editor so that you can start filling it out.
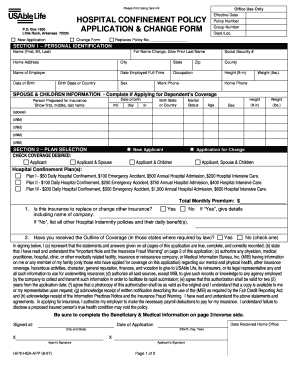
- Begin with Section 1 – Personal Identification. Fill in your first name, middle initial, and last name. Provide your home address, including city, state, zip code, and county. Include your contact number and work phone.
- Next, provide your social security number, occupation, and the name of your employer. Include the date you were employed full-time and your birth state or country. Add your height and weight in the provided fields.
- If you are applying for dependent coverage, complete the Spouse & Children Information section. List the names, dates of birth, height, weight, marital status, and sex for each person you are including.
- Proceed to Section 2 – Plan Selection. Indicate whether this is a new application or a change. Select the desired coverage option (e.g., Applicant, Applicant & Spouse) and choose the hospital confinement plan that fits your needs.
- Answer the questions about prior insurance coverage and whether you've reviewed the Outline of Coverage. Ensure you provide details where necessary.
- In Section 3 – Beneficiary, fill in the details for the beneficiary including their name, birthdate, and relationship to you. Indicate if they are a primary or secondary beneficiary and specify the percentage if applicable.
- Complete Section 4 – Medical Information by answering all health-related questions regarding any proposed insured persons. Provide details if any medical conditions are relevant.
- Finally, review all the information to ensure accuracy. Once complete, you will have options to save your changes, download, print, or share the completed form.
Start filling out your Hospital Confinement Policy Application & Change Form online today!
Coverage. Benefit can be used any way the insured chooses – to cover additional medical expenses or for any other out-of-pocket costs. Benefits are paid directly to the insured. Plan pays up to $150/day upon discharge for hospitalizations over three days paid in addition to any other insurance.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.