Get Ca Edward Diao New Workers Compensation Intake Form Only
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CA Edward Diao New Workers Compensation Intake Form ONLY online
Filling out the CA Edward Diao New Workers Compensation Intake Form is crucial for ensuring that your workers' compensation claim is processed efficiently. This guide will walk you through each step of completing the form online, addressing every necessary field to help you provide the required information accurately.
Follow the steps to complete the intake form online:
- Click ‘Get Form’ button to obtain the form and open it in the editor.
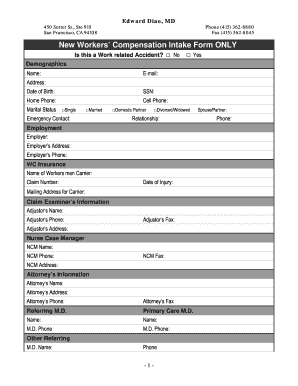
- Begin by indicating whether the incident was work-related by selecting either 'Yes' or 'No' for the question at the top of the form.
- Proceed to fill out the demographic information section, including your name, email, address, date of birth, social security number, home phone, and cell phone.
- Indicate your marital status by selecting from the options provided (single, married, domestic partner, divorced/widowed). Enter an emergency contact and their relationship to you.
- In the employment section, provide your employer's name, address, and phone number, as well as the details of the workers' compensation insurance carrier and any claim number.
- Fill out the claim examiner's information, including the adjustor’s name, phone, fax, and address.
- Include information regarding your nurse case manager (NCM) if applicable, detailing their name, phone, fax, and address.
- Input any attorney information, if you have one, including the name, address, phone, and fax number.
- Detail your current injury by providing your age, dominant hand, height, weight, and a description of the injury. Explain how the injury occurred and how it affects your daily work and living activities.
- List your past medical and surgical history, current medications, and any allergies.
- Complete the social history section by noting your hobbies or interests and alcohol and tobacco use.
- Review the health and family health history questions, selecting appropriate responses.
- Read the financial policy and controlled substances agreement carefully before signing.
- Once you have completed all sections, you can save changes, download, print, or share the form as needed.
Complete the CA Edward Diao New Workers Compensation Intake Form online to ensure your claim is processed swiftly and accurately.
Form CA-7 is also used to claim leave buy back, schedule award or lost pay elements (ie, night differential, Sunday premium, holiday pay, etc). Form CA-7 should be submitted by an injured worker (IW) every two weeks while disabled and in a LWOP status, unless the IW has been placed on the periodic roll.