Loading
Get Dol Owcp-1500 2006
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the DoL OWCP-1500 online
This guide provides a clear and supportive approach to filling out the DoL OWCP-1500 form online. Follow these detailed steps to ensure that your health insurance claim form is completed accurately and efficiently.
Follow the steps to complete your DoL OWCP-1500 form online.
- Press the ‘Get Form’ button to access the OWCP-1500 form and open it in the designated online editor.
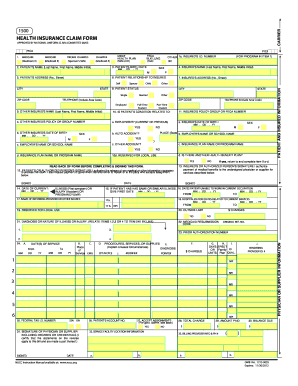
- In Section 1a, enter the patient's claim number when prompted. This is essential for processing your claim.
- In Section 2, provide the patient's full name, including last name, first name, and middle initial.
- For Section 3, input the patient's date of birth using the specified format (MM/DD/YY) and mark the corresponding sex box.
- In Section 4, leave this blank for FECA claims. If applicable under BLBA or EEOICPA, enter the name of the party to whom medical payment is due.
- Fill in Section 5 by providing the patient’s complete address including street, city, state, and ZIP code. A telephone number is optional.
- Leave Sections 6 to 9 blank unless instructed otherwise in the guidelines provided.
- In Section 10, briefly indicate if the patient's condition relates to any of the mentioned circumstances.
- Complete Section 11 with the patient's claim number for FECA. This is crucial to avoid delays in processing.
- Follow instructions through Sections 12 to 24, entering required details such as diagnoses, dates of service, charges, and providing the physician's signature.
- Once all fields are completed accurately, review the form for any omissions or errors.
- Finalize the process by saving changes, downloading the completed form, printing it, or sharing it as required for submission.
Complete your DoL OWCP-1500 form online today to ensure timely processing of your health insurance claims.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
To obtain CMS 1500 forms, you can download them directly from the Centers for Medicare & Medicaid Services website. Alternatively, uslegalforms provides easy access to these forms and can assist you with associated processes. Ensure that when you use these forms, you properly complete the details to support your OWCP claims effectively. Having the right resources will guide you through the necessary steps.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.