Loading
Get Oh Odm 10207 2021-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the OH ODM 10207 online
This guide provides clear and supportive instructions on how to complete the OH ODM 10207 form online. The process is straightforward and designed to assist users in accurately filling out essential information regarding pregnancy risk assessments.
Follow the steps to accurately complete the form online.
- Click ‘Get Form’ button to access the form and open it in the editor.
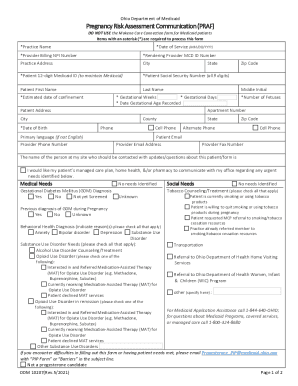
- *Practice Name: Enter the name of the practice providing the service.
- *Date of Service: Fill in the date when the service was rendered in MM/DD/YYYY format.
- *Provider Billing NPI Number: Input the National Provider Identifier for billing purposes.
- *Rendering Provider MCD ID Number: Enter the Medicaid ID number of the provider delivering the service.
- Practice Address: Provide the complete address of the practice.
- City: Specify the city where the practice is located.
- *Patient 12-digit Medicaid ID: Fill in the patient’s Medicaid ID number to ensure proper Medicaid processing.
- *Patient Social Security Number: Enter the full 9-digit Social Security number of the patient.
- Patient First Name: Provide the first name of the patient.
- Last Name: Enter the last name of the patient.
- *Estimated Date of Confinement: Input an estimated date for the patient’s delivery.
- State: Fill in the state of the practice.
- Middle Initial: Enter the middle initial of the patient, if applicable.
- *Gestational Weeks: Specify the number of weeks the patient is currently gestating.
- *Gestational Days: Indicate the number of days since the last completed week of gestation.
- *Date Gestational Age Recorded: Fill in the date when the gestational age was last assessed.
- Patient Address: Provide the address where the patient resides.
- *Number of Fetuses: Input the total number of fetuses being carried.
- Apartment Number: Include the apartment number, if applicable.
- City: Specify the city of the patient's residence.
- County: Enter the county where the patient lives.
- *Date of Birth: Fill in the patient's date of birth.
- Zip Code: Include the zip code of the patient’s residence.
- Phone: Provide a primary contact phone number for the patient.
- Cell Phone: Enter a cell phone number for quick communication.
- Primary Language: Indicate the primary language spoken by the patient, if not English.
- Provider Phone Number: Provide the phone number of the provider’s office.
- State: Specify the state of the provider’s address.
- Zip Code: Enter the zip code of the provider’s office.
- Alternate Phone: Include an alternative phone number for the provider’s office.
- Cell Phone: Enter a cell phone number for the provider’s office.
- Patient Email: Provide the email address of the patient.
- Provider Email Address: Enter the email address for the provider.
- Provider Fax Number: Include the fax number for the provider’s office.
- Contact Person: Specify the name of the person who should be contacted about this form.
- Managed Care Communication: Indicate if the patient's managed care plan should communicate with the practice regarding urgent needs.
- Medical Needs: Check the appropriate box for any medical needs identified.
- Behavioral Health Diagnosis: Indicate any behavioral health diagnoses applicable.
- Social Needs: Check the relevant options for any social needs.
- Opioid Use Disorder in Remission: Specify if applicable and check the appropriate box.
- Final Review: Review all entries for accuracy before proceeding.
- Save Changes: Ensure to save any changes made to the form.
- Download or Print: Users can download or print the completed form as needed.
- Share the Form: After completion, share the form as necessary.
Complete your OH ODM 10207 form online now to ensure accurate and timely submissions.
Eligibility levels for parents are presented as a percentage of the 2023 FPL for a family of three, which is $24,860. Eligibility limits for single adults without dependent children are presented as a percentage of the 2023 FPL for an individual, which is $14,580.