Get Futurecomp Accident Reporting Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the FutureComp Accident Reporting Form online
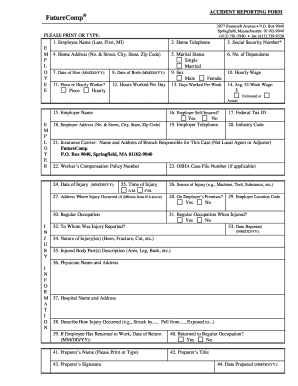
Completing the FutureComp Accident Reporting Form online is an essential process for reporting workplace injuries effectively. This guide will walk you through each section of the form to ensure that you provide the necessary information clearly and accurately.
Follow the steps to complete the FutureComp Accident Reporting Form online.
- Click ‘Get Form’ button to access the form and open it in your digital editor.
- Begin with entering the employee's full name in the designated fields for the last name, first name, and middle initial. This information is crucial for accurately identifying the individual affected by the incident.
- Provide the employee's home telephone number to ensure you can be contacted for follow-up information. Additionally, input their Social Security number in the appropriate field.
- Complete the home address section with the street number and name, city, state, and zip code, ensuring each part is accurate for correspondence.
- Indicate the employee’s marital status by selecting 'Single' or 'Married' from the options. Fill in the number of dependents and the employee's date of hire in the specified format.
- Enter the employee's date of birth, hourly wage, and average 52-week wage, ensuring clarity in whether the amount provided is estimated or actual.
- Fill in the employer's name and address, including the federal tax ID number if available. Specify whether the employer is self-insured.
- Detail the nature of the incident by recording the date and time of the injury, along with the source of the injury and its location.
- Describe the nature of the injury, including body parts affected, and provide information about the physician and hospital if treatment was received.
- Upon completion, review all entries for accuracy. Save changes to the form in your editor, then download, print, or share the document as necessary for submission.
Start completing your FutureComp Accident Reporting Form online today!
When filling out a DWC 1 form, start by entering your personal information, including your name, address, and occupation. Next, detail the injury specifics, like when and how it happened, and any witnesses present. The FutureComp Accident Reporting Form can help you gather all relevant information before completing the DWC 1, reducing the risk of errors. Ensuring accuracy is critical to the success of your workers' compensation claim.