Loading
Get Personal Needs Allowance (pna) Account Remittance Notice
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the PERSONAL NEEDS ALLOWANCE (PNA) ACCOUNT REMITTANCE NOTICE online
Filling out the Personal Needs Allowance Account Remittance Notice is a crucial process in managing the finances of deceased residents under Ohio's Medicaid program. This guide will walk you through each section of the form, ensuring you have the necessary information to complete it accurately online.
Follow the steps to complete this important form.
- Click ‘Get Form’ button to obtain the form and access it in your preferred online editor.
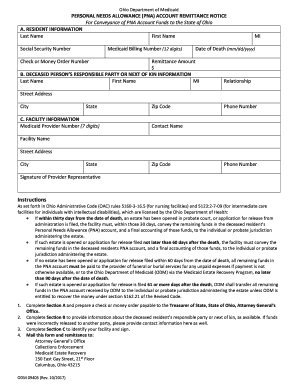
- In Section A, enter the following resident information: Last name, first name, social security number, Medicaid billing number (12 digits), check or money order number, middle initial, date of death (formatted as mm/dd/yyyy), and the remittance amount. Make sure the information is correct to avoid processing delays.
- Proceed to Section B to fill in the details of the deceased person's responsible party or next of kin. Provide the last name, first name, middle initial, relationship to the deceased, street address, city, state, and any other relevant contact information.
- In Section C, include the facility information by providing the Medicaid provider number (7 digits), zip code, phone number, contact name, facility name, street address, city, state, zip code, and another phone number if applicable.
- Ensure the form has been signed by a provider representative to validate the submission. Review all sections for completeness and accuracy.
- Once completed, take a moment to review the entire form for any errors. After confirming the accuracy, save the changes and prepare to send the form.
- Finally, mail this form along with the remittance to the specified address: Attorney General’s Office, Collections Enforcement, Medicaid Estate Recovery, 150 East Gay Street, 21st Floor, Columbus, Ohio 43215.
Start completing your PERSONAL NEEDS ALLOWANCE (PNA) ACCOUNT REMITTANCE NOTICE online to ensure prompt processing.
The Personal Needs Allowance (PNA) is the monthly sum of money that residents who receive Medicaid may retain from their personal income. Any income above the allowance is applied toward the cost of their care.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.