Loading
Get 18553953248
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the 18553953248 online
Filling out the 18553953248 Benefits Investigation Form for ® (aflibercept) injection can be straightforward with the right guidance. This guide will lead you through the necessary steps to ensure your form is completed accurately and efficiently.
Follow the steps to successfully complete the form.
- Press the 'Get Form' button to access the Benefits Investigation Form and open it for editing.
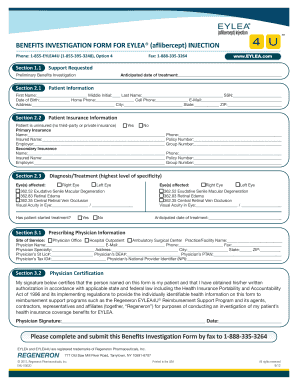
- Begin with Section 1.1, where you indicate the support requested. Check the box for 'Preliminary Benefits Investigation.'
- In Section 2.1, fill in the anticipated date of treatment and enter all required patient information, including first name, middle initial, last name, social security number, date of birth, home phone, cell phone, email address, and complete address.
- Proceed to Section 2.2, which involves patient insurance information. Indicate whether the patient is uninsured. If they have primary or secondary insurance, provide the necessary details including the name of the insurance company, the phone number, insured name, policy number, employer, and group number.
- In Section 2.3, specify the affected eye(s) and the diagnosis/treatment. Provide the visual acuity for each eye affected and indicate if treatment has already started.
- Next, in Section 3.1, repeat the entry for affected eye(s) and diagnosis/treatment as specified in the previous section. Include the anticipated date of treatment and complete the prescribing physician information, including site of service, physician office or facility name, contact details, and specialties.
- In Section 3.2, the prescribing physician must provide their signature and date to certify the patient's information. Ensure that the physician's signature is obtained along with any necessary credentials.
- Finally, review all entered information for accuracy, then save your changes. Once you have confirmed that the form is complete, you can download, print, or share the Benefits Investigation Form as required.
Start filling out your 18553953248 form online today to ensure timely assistance.
About The Commercial Copay Card Program If you have commercial insurance, you may be eligible to pay as little as $0 for each treatment.*,† You may qualify for copay assistance if: 1. You have commercial or private insurance that covers . 2. You are receiving for an FDA-approved indication.