Loading
Get Green Mountain Support Services - Medication Administration Record
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Green Mountain Support Services - Medication Administration Record online
The Green Mountain Support Services - Medication Administration Record is a vital document for tracking medication administration. This guide provides clear, step-by-step instructions to assist users in accurately completing this form online.
Follow the steps to successfully complete the Medication Administration Record.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
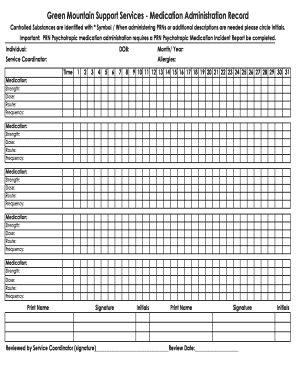
- Begin by entering the individual's details, including their name, date of birth (DOB), and designated service coordinator.
- In the space provided, input the medication details. For each prescribed medication, include the following: medication name, strength, dosage, route of administration, and frequency of dosing.
- For controlled substances, ensure to identify them with the asterisk (*) symbol and note any additional information by circling initials where necessary.
- If administering PRN (as needed) medications, circle the respective initials and remember that a PRN Psychotropic Medication Incident Report must be filled out for these medications.
- Document any allergies the individual may have in the designated section to ensure safety during medication administration.
- At the bottom of the form, print your name, provide your signature, and initial the form to indicate your review and agreement.
- A service coordinator is required to review the completed record. They will sign and date the form, confirming that the information is accurate.
- Once all sections are complete, you can save changes, download, print, or share the completed form based on your needs.
Complete your documents online today for efficient medication management.
The medication administration record includes the patient name, full name of medication, administration time, dose, route, frequency, site of administration for parenteral medications, and the nurses' initials, signatures and (possibly) the prescribing health care provider.