Get Il Hfs 3701h 2008-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the IL HFS 3701H online
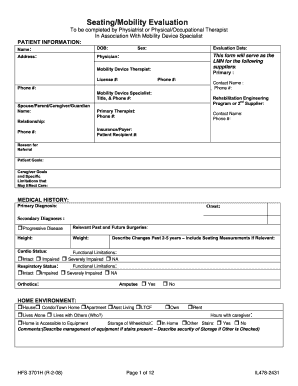
The IL HFS 3701H is a crucial document for health professionals conducting a seating and mobility evaluation. Properly filling out this form is essential to ensure that individuals receive the appropriate mobility devices and support. This guide will walk you through the process of completing the form online, section by section.
Follow the steps to accurately fill out the IL HFS 3701H online.
- Click ‘Get Form’ button to access the IL HFS 3701H and open it in your online document editor.
- Begin by filling in the 'Patient Information' section. Include the patient's name, date of birth, sex, address, physician’s name, and evaluation date. Ensure that all details are accurate to assist in the evaluation process.
- Next, complete the section for 'Mobility Device Specialist'. Input the specialist’s name, license number, and contact information. This section is vital for communication with the mobility device provider.
- In the 'Medical History' section, provide primary and secondary diagnoses, onset dates, height, weight, and a brief overview of functional limitations. It's important to note any significant medical history that may impact mobility.
- Fill out the 'Home Environment' part by indicating the type of living situation and whether the home is accessible for wheelchair use. Specify any details about stairs or other challenges.
- In the 'Community ADL' section, detail transportation methods and identify any additional mobility requirements specific to the patient’s activities of daily living.
- Proceed to 'Functional/Sensory Processing Skills' and assess the patient's handedness, visual acuity, and communication abilities. Note any limitations to ensure thorough evaluation related to wheelchair operation.
- In the 'Current Seating / Mobility' section, provide details about the current mobility base and seating system, including the model and any relevant modifications, ensuring to describe the current condition.
- Complete the 'Recommendations & Justification' portion by justifying the need for specific mobility equipment based on the completed assessments. Clearly articulate why chosen equipment is appropriate.
- Finally, ensure all signatures are obtained in the 'Signatures' section. This includes signatures from the patient or caregiver, therapist, supplier, and physician. Review the entire document for any missing information before submission.
- After completing the form, you can save your changes, download the document, print it for physical submission, or share it with relevant parties.
Start filling out the IL HFS 3701H online now to ensure timely and accurate processing of mobility device evaluations.
Related links form
Receiving an EDI payment indicates that the Illinois Department of Healthcare and Family Services processed a transaction related to services you provided or received. This payment is designed to ensure that reimbursements are delivered quickly and accurately, reflecting the services billed under programs like IL HFS 3701H. If you have questions about specific payments, platforms like UsLegalForms can help clarify the details and assist you further.