Loading
Get This Form Must Be Completed By A Physician Or Clinician.
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the This Form Must Be Completed By A Physician Or Clinician. online
Filling out the This Form Must Be Completed By A Physician Or Clinician accurately is essential for ensuring that youth receive the necessary mental health support. This guide provides step-by-step instructions to help physicians and clinicians complete the form efficiently and correctly.
Follow the steps to fill out the form online:
- Use the ‘Get Form’ button to access the form and open it in your preferred online document editor.
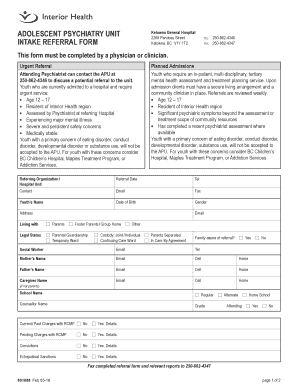
- Start by entering the referring organization or hospital unit details. Make sure you provide accurate referral date, telephone number, contact name, and email.
- Input the youth’s name, date of birth, gender, and address. Provide the youth's email and specify who they are living with.
- Specify the legal status selecting options from parental guardianship, temporary ward, or other categories as applicable.
- Indicate if the family is aware of the referral by checking 'Yes' or 'No'.
- Complete the fields regarding the social worker if applicable, and fill in the details of the youth's parents or caregivers.
- Provide the school name and the grade the youth is attending, marking if they are in a regular, alternate, or home school.
- Indicate any current or past charges with the RCMP and provide details if applicable.
- Check if the youth has seen a psychiatrist and provide their name, while indicating previous appointments and any significant medical concerns.
- Detail the presenting concerns and provide a description of the issues the youth is facing.
- State the reasons for referral, selecting from diagnostic clarification, treatment planning, or other specified reasons.
- List any medications the youth is currently taking or has taken in the past, including dosage and duration.
- Indicate if relevant reports or assessments will be included and explain if any are missing.
- Once the form is fully completed, save your changes, and choose to download, print, or share the form as needed.
Complete the necessary documents online today to ensure timely support for youth in need.
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.