Loading
Get Patient Application Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Patient Application Form online
Completing the Patient Application Form online is an essential step toward receiving personalized healthcare. This guide will walk you through each section of the form, ensuring that you provide the necessary information accurately and efficiently.
Follow the steps to complete the Patient Application Form online.
- Click ‘Get Form’ button to obtain the form and open it in the online editor.
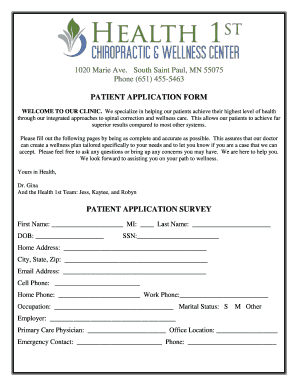
- Begin filling out the personal information section, which includes your first name, middle initial, last name, date of birth, and social security number. Be sure to double-check for accuracy.
- Provide your contact details. This includes your home address, city, state, zip code, email address, and phone numbers (cell, home, and work). It's important that this information is up-to-date for effective communication.
- In the occupational information section, input your occupation, marital status, and employer. This helps in understanding your work-life balance and how it may affect your health.
- List your primary care physician and their office location. This assists the clinic in coordinating any necessary referrals.
- Fill out the emergency contact section with a name and phone number for someone who can be reached in case of an emergency during your visit.
- In the 'Purpose of this Visit' section, specify your main complaint and answer questions related to any accidents or injuries related to this visit.
- Indicate the type and nature of your pain, and how often you experience these symptoms. Be honest in your assessment to ensure appropriate care.
- Fill in your health and lifestyle details, including exercise habits, smoking and alcohol consumption, and any supplements or medications you take.
- Review the health conditions list and check any that apply to you. This information is crucial for your health evaluation.
- On the goals for care section, indicate any health concerns or interests you have regarding your wellbeing.
- Read and understand the terms of acceptance and the medical information release authorization. You must provide your initials where prompted to indicate acceptance.
- Complete the financial agreement and provide necessary information about your insurance, ensuring a smooth billing process.
- Once you have filled out all sections, review your entries carefully. Make sure all information is complete and accurate.
- Finally, save your changes, download a copy for your records, and print or share the form as required.
Start filling out your Patient Application Form online today and take the first step toward better health.
A patient information form is used by medical practices to collect information from patients. Use this free Patient Information Form template to collect patients' contact information, insurance details, and any other information you need!
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.