Loading
Get Hospital Forms 8850134 2005-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Hospital Forms 8850134 online
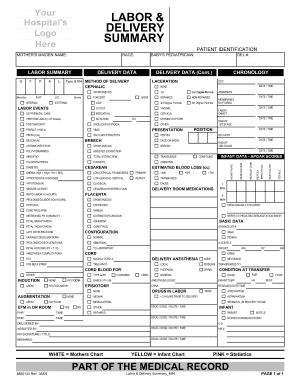
Filling out the Hospital Forms 8850134 online is crucial for effective record-keeping during labor and delivery. This guide provides a step-by-step approach tailored to assist you in completing this important document accurately and efficiently.
Follow the steps to fill out Hospital Forms 8850134 accurately online.
- Press the ‘Get Form’ button to acquire the Hospital Forms 8850134 and open it in the designated editor.
- Begin by providing the patient's identification, including their race and other relevant demographic information.
- Move to the method of delivery section. Indicate whether the delivery was vaginal or cesarean, and note any lacerations or complications experienced during the procedure.
- Detail the labor events, including prenatal care information, onset of labor, and any specific complications, such as preterm labor, that were noted.
- Fill out the infant data, paying close attention to APGAR scores, estimated blood loss, and any necessary neonatal details.
- Complete the anesthesia section, indicating the types used during delivery and any complications that arose.
- Double-check all sections for accuracy, then save your changes to the form.
- Finally, download or print the completed Hospital Forms 8850134 for your records, or share it as necessary.
Start completing your Hospital Forms 8850134 online today!
Filling out a medical necessity form requires you to include your personal information and a detailed description of your medical condition and why treatment is essential. Be prepared to support your claims with medical documentation if necessary. By using Hospital Forms 8850134, you can access user-friendly forms that clarify expectations and make your submission easier.