Get Valueoptions Outpatient Discharge Form 2008-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the ValueOptions Outpatient Discharge Form online
Completing the ValueOptions Outpatient Discharge Form is a crucial step in ensuring the successful discharge of a patient from outpatient services. This guide provides clear and supportive instructions for filling out the form accurately and efficiently online.
Follow the steps to complete the form successfully.
- Press the ‘Get Form’ button to obtain the form and open it for editing.
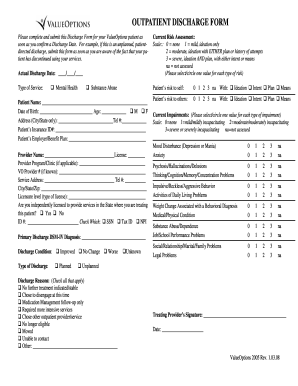
- Enter the actual discharge date in the designated field. Make sure to select the correct date format.
- Indicate the type of service provided by selecting either ‘Mental Health’ or ‘Substance Abuse’.
- Fill in the patient’s information, including their name, date of birth, age, address (City/State), and telephone number.
- Provide the patient’s insurance ID number and their employer or benefit plan details.
- Complete the provider's information by entering their name and license number, as well as the program or clinic they represent, if applicable.
- If known, fill in the VO provider number and the service address along with its contact number and complete city/state/zip information.
- Specify the licensure level and confirm whether the provider is independently licensed to deliver services in the state.
- Select the primary discharge DSM-IV diagnosis from the available options provided.
- Indicate the discharge condition by selecting one of the options: 'Improved', 'No Change', or 'Worse'.
- Select the type of discharge by checking whether it is 'Planned' or 'Unplanned'.
- Conduct a current risk assessment by selecting the appropriate scale values for the patient’s risk to self and others.
- Evaluate current impairments, circling the value that best represents each type of impairment based on the given scale.
- Check the reasons for discharge by selecting all the applicable options listed.
- Obtain the treating provider’s signature and date the form to finalize it.
- Once completed, save changes, download, print, or share the form as needed.
Complete your ValueOptions Outpatient Discharge Form online today to streamline the discharge process.
A patient discharge letter is a formal document provided to patients at the conclusion of their outpatient treatment. It includes critical information about their care, instructions for post-treatment, and any necessary referrals for further evaluation. This letter serves as a guide for patients as they transition away from direct medical care. To enhance understanding and clarity, the ValueOptions Outpatient Discharge Form can be an excellent resource.