Loading
Get Va Vwc 3 2008-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the VA VWC 3 online
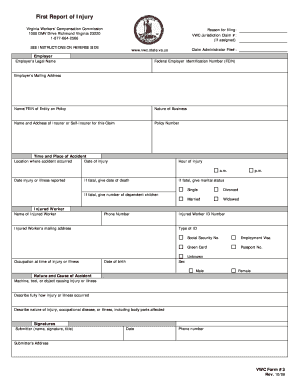
The Virginia Workers' Compensation Commission requires the VA VWC 3 form for reporting workplace injuries. This guide will provide detailed instructions on how to complete this form online to ensure accurate and timely submissions.
Follow the steps to successfully complete the VA VWC 3 form online.
- Click ‘Get Form’ button to download the VA VWC 3 form and open it in the editor.
- Begin by filling in the section labeled 'Employer'. Enter the employer’s legal name, Federal Employer Identification Number (FEIN), and their mailing address. Additionally, include the name and FEIN of the entity on the policy, the nature of the business, and the insurer or self-insurer information, including the policy number.
- In the 'Time and Place of Accident' section, provide the date and location of the injury, alongside the hour of the injury. Specify whether it occurred in the a.m. or p.m., and indicate the date injury or illness was reported. If the injury is fatal, include the date of death.
- For the 'Injured Worker' section, enter the name and phone number of the injured worker. Specify their ID number, type of identification, mailing address, Social Security number, and employment status (visa, green card, or passport). Don’t forget to input their occupation at the time of injury, date of birth, and sex.
- In the 'Nature and Cause of Accident' section, describe the machine, tool, or object that caused the injury. Provide a detailed description of how the injury or illness occurred, along with the nature of the injury, occupational disease, or illness, including body parts affected.
- Complete the 'Signatures' section by entering the submitter's name, signature, title, date, phone number, and their address. Ensure all information is accurate before proceeding.
- Once all sections are completed, review the form for accuracy. After ensuring everything is correct, save your changes. You can then download, print, or share the form as needed.
Submit your VA VWC 3 form online to ensure prompt processing of your workplace injury claim.
Related links form
You cannot sue your employer for a work-related injury if you are receiving workers' comp benefits; however, you can pursue your claim while maintaining your employment. Workers' comp is designed to provide benefits instead of a lawsuit in exchange for forfeiting the right to sue. If you still want to explore your options, consider consulting resources like UsLegalForms for comprehensive guidance.